Thoracic Radiculopathy

Medically Reviewed By:
Thoracic radiculopathy refers to nerve-related issues affecting the thoracic spine (mid-back) and the nerves branching from this area. This condition may contribute to radiating discomfort or unusual sensations in regions served by these nerves. Although often considered uncommon, clinical insights suggest that it may be more frequently observed than previously recognized.
This overview explores thoracic radiculopathy, covering key aspects of diagnosis and treatment based on comprehensive clinical perspectives.
What Is Thoracic Radiculopathy?

Thoracic radiculopathy develops when one or more spinal nerves in the thoracic spine—the middle section of the spine in the upper back—become compressed, irritated, or pinched. This region provides stability for the upper body while allowing controlled movement. When a nerve is affected, discomfort may radiate from the upper back to the torso, chest, or abdomen.
Radiculopathy occurs when a spinal nerve does not function properly, which may contribute to sharp or burning pain, numbness, tingling, or muscle weakness in the areas served by the affected nerve. Thoracic radiculopathy is less common than cervical radiculopathy (which affects the neck) or lumbar radiculopathy (which affects the lower back).
The thoracic spine’s connection to the rib cage increases its stability, making it less prone to disc-related issues or degenerative changes that often lead to radiculopathy in other spinal regions. Because of this, thoracic nerve pain occurs less frequently. However, its symptoms can be difficult to diagnose and manage due to their varied presentation.
Causes Of Thoracic Radiculopathy
Various conditions can compress or irritate nerve roots in the thoracic spine, potentially leading to discomfort, tingling, numbness, or muscle weakness. Common causes include:
Disc Bulge
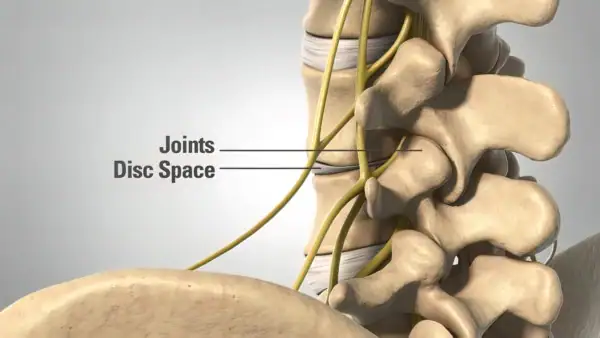
A disc bulge occurs when a spinal disc shifts out of place between vertebrae. These discs cushion the spine and support movement, but when they extend into the small openings (foramina) where spinal nerves exit, they may cause nerve irritation or compression.
In the thoracic spine, a bulging disc can compress or irritate nearby nerve roots, potentially leading to numbness, weakness, or discomfort in the areas served by the affected nerves.
The facet joints, which connect the vertebrae, sit close to these nerve roots and can also undergo degenerative changes over time. When a bulging disc occurs alongside facet joint degeneration, nerve compression may increase, contributing to thoracic radiculopathy symptoms.
Arthritis In The Facet Joint
Facet joint arthritis, also called facet joint arthropathy, can affect any part of the spine, including the thoracic region. Facet joints are small, paired joints at the back of each vertebra that support flexibility and stability.
Over time, these joints may deteriorate due to wear and tear, which can lead to arthritis. In the thoracic spine, this can narrow spaces around spinal nerves (foraminal stenosis), potentially contributing to nerve compression and thoracic radiculopathy symptoms. Facet joint arthritis may also limit spinal mobility, causing stiffness and discomfort.
Muscle Atrophy
Muscle atrophy, or the weakening and shrinking of muscles, can contribute to thoracic radiculopathy by reducing spinal stability. The multifidus and rotatores muscles help maintain vertebral alignment, but aging, injury, inactivity, or degenerative conditions can cause them to weaken.
As these muscles lose strength, the thoracic vertebrae may shift slightly, narrowing the spaces where spinal nerves exit. This added pressure can contribute to nerve irritation or compression, potentially leading to thoracic radiculopathy symptoms such as pain, tingling, or numbness in affected areas.
Compression Fracture
A compression fracture in the thoracic spine can contribute to thoracic radiculopathy. This type of fracture occurs when excessive pressure causes a vertebra to collapse into a wedge-like shape. Common causes include osteoporosis, trauma, or conditions that weaken bone structure, such as metastatic cancer.
When a vertebra compresses, it may narrow the spinal canal or foramina, potentially irritating or compressing nearby nerve roots. This can lead to thoracic radiculopathy symptoms. The resulting instability may further increase nerve compression, contributing to discomfort and mobility limitations.
Bone Spurs (Osteophytes)
Bone spurs are bony projections that develop along the edges of bones, often due to joint degeneration or instability. In the thoracic spine, they can form on the vertebrae or around the facet joints, commonly as a result of osteoarthritis. While these spurs help stabilize weakened joints, they may become problematic if they press on nearby spinal nerves.
When osteophytes narrow the foramina or encroach on the spinal canal, they can contribute to nerve compression and thoracic radiculopathy symptoms. The severity and specific symptoms depend on the location and size of the bone spur, ranging from mild discomfort to functional limitations.
Other Factors To Consider
Beyond direct spinal conditions, certain factors may increase susceptibility to nerve compression or irritation in the thoracic spine. These include:
- Age: Spinal degeneration causes disc dehydration, joint wear, and bone loss, increasing the risk of bone spurs, herniated discs, or compression fractures that may affect nerves.
- Obesity: Excess weight adds strain to the spine, accelerating disc and joint degeneration. This pressure may increase the likelihood of nerve compression in the thoracic region.
- Repetitive Strain or Trauma: Repetitive movements or trauma from falls, accidents, or sports can weaken spinal structures, potentially leading to fractures, disc damage, or nerve irritation.
Symptoms Of Thoracic Spine Nerve Damage
Thoracic spine nerve damage often causes upper back pain that radiates around the torso, sometimes reaching the rib cage’s side or front. Pain may feel sharp, dull, or electric, depending on the severity and cause.
In some cases, thoracic radiculopathy may cause abdominal discomfort. Irritated nerves in the lower thoracic region can send pain signals along the abdomen, sometimes mimicking digestive issues. This radiating pain may feel like a band across the belly, which can lead to diagnostic confusion.
Additional symptoms include:
- Weakness in the legs: Impaired nerve function may weaken leg muscles, affecting stability and weight-bearing ability.
- Loss of coordination: Nerve compression can disrupt reflexes and precise movements, making coordination more difficult.
- Mid-back pain: Inflammation or nerve compression can cause dull, aching, or sharp pain that worsens with movement.
- Numbness or tingling: Sensations may occur in the back, chest, abdomen, or legs, depending on which nerve roots are affected.
Diagnosis Of Thoracic Radiculopathy
Thoracic radiculopathy is less common than cervical or lumbar radiculopathy, making diagnosis more challenging. A thorough evaluation of the thoracic spine is essential and typically involves a clinical assessment, imaging studies, and additional diagnostic techniques when needed.
Diagnosis usually includes a medical history review, physical exam, and thoracic MRI. MRI imaging helps identify disc bulges, arthritis, or other structural changes that may contribute to nerve compression. However, even with MRI, diagnosing thoracic radiculopathy can be complex.
Limited experience with this condition or incomplete evaluations may lead to delayed or missed diagnoses. A careful, comprehensive approach is crucial for accurate identification and appropriate management.
Clinical Examination
A physical exam plays a key role in diagnosing thoracic radiculopathy. Physicians assess range of motion, reflexes, and neurological function to identify signs of nerve involvement. A pinwheel tool is often used to evaluate sensory response by rolling it along the upper back. Changes in sensation, such as numbness or heightened sensitivity, may indicate nerve irritation.
Despite its usefulness, this sensory test is not routinely performed by many specialists, highlighting a gap in standard thoracic radiculopathy evaluations.
Thoracic MRI
A thoracic MRI provides detailed images of the spine, helping identify conditions such as herniated discs, bone spurs, and spinal stenosis that may contribute to thoracic radiculopathy. It also helps rule out fractures or other structural issues, supporting a more accurate diagnosis.
Symptom location can guide MRI analysis by pinpointing the affected thoracic level. Matching MRI findings with symptoms helps identify potential nerve irritation sources. However, few physicians conduct a thorough thoracic evaluation, including symptom correlation with spinal levels.
Common Treatment Options To Manage Thoracic Radiculopathy
Initial treatment often includes conservative approaches, such as physical therapy and medications, to improve spinal alignment, reduce inflammation, and strengthen supporting muscles. While these methods are effective for many, some cases may require more targeted interventions.
The thoracic spine’s proximity to the lungs makes certain procedures, like injections and surgeries, more technically complex. As a result, fewer physicians specialize in thoracic-specific techniques, which may limit access to advanced treatments. However, most individuals experience significant relief with conservative care alone.
Common treatment options include:
- Physical therapy: Exercises and techniques that improve posture, flexibility, and strength to reduce nerve compression and support spinal health.
- Discectomy: A procedure that removes part of a herniated disc pressing on a nerve to relieve symptoms and reduce compression.
Regenexx Approach With Minimally Invasive Procedures
Physicians in the licensed Regenexx network take a specialized approach to treating thoracic radiculopathy by focusing on procedures that may help address symptoms and improve function without surgery.
Procedures using Regenexx injectates utilize a patient’s own blood or bone marrow to support the body’s natural healing process. This approach aims to promote recovery while reducing the risks associated with traditional surgical interventions, offering a non-surgical alternative.
Regenexx SCP Injectate
Procedures using Regenexx SCP injectate involve a highly refined form of platelet-rich plasma (PRP). Blood is drawn and processed to concentrate platelets and growth factors, which are then injected using imaging guidance for precision. Regenexx SCP injectate provides a higher concentration of growth factors compared to standard PRP preparations.
Regenexx SD Injectate
Procedures using Regenexx SD injectate follow a patented protocol that processes Bone Marrow Concentrate (BMC), which contains the patient’s own cells. Regenexx lab processing routinely achieves a concentration up to 20 times higher than standard methods.
A Sample Case Study On How PRP Helps
Brad, a young adult with a 20-year history of upper back pain from a high school wrestling injury, experienced periodic flare-ups with wrap-around pain worsened by breathing. His MRI revealed disc bulges at T6-T7 and T7-T8. A clinical examination showed decreased sensation and rib tenderness, suggesting thoracic nerve involvement.
Rather than using steroid injections, which may reduce inflammation but contribute to tissue breakdown, Brad received a PRP injection from his own blood. It targeted the disc bulge, surrounding fascial tissue, and weakened stabilizing muscles. Using X-ray and ultrasound guidance, the physician precisely placed the injection to address multiple pain sources.
To learn more about orthobiologics such as PRP, view the video below:
After a single PRP injection, Brad reported significant improvement. By three to four months post-treatment, he could engage in physically demanding activities, such as lifting heavy objects, without pain. This case highlights how PRP may help manage symptoms in some individuals when applied with the right expertise and regenerative approach.
Discover Approaches For Managing Thoracic Radiculopathy
Though less common, thoracic radiculopathy can significantly impact daily life. Management options range from conservative therapies to procedures using Regenexx injectates, such as PRP and bone marrow concentrate injections.
Procedures using Regenexx lab processes support the body’s natural healing response, offering a non-surgical approach to reducing pain and improving function.
Struggling with thoracic radiculopathy? Learn how a physician in the licensed Regenexx network may be able to help address your thoracic radiculopathy.
Get started to see if you are a Regenexx candidate
To talk one-on-one with one of our team members about how the Regenexx approach may be able to help your orthopedic pain or injury, please complete the form below and we will be in touch with you within the next business day.
Medically Reviewed By: