Avoid Ulnar Shortening Surgery: What’s Causing My Pain if It’s Not My Ulna Bone?
A few years back, I blogged on the barbaric procedure known as ulnar shortening. A patient who was about to pull the trigger on this surgery wrote me and wanted me to blog on what could be causing the pain he experiences. Hence, this morning’s blog.
What Is Ulnar Variance or a Long Ulna?
The forearm has two bones—one is the ulna and the other the radius. The main idea here is that someone is born with a long ulna bone and that this causes too much force on the little-finger side of the wrist, leading to arthritis and soft-tissue injury. All of this eventually causes pain, which leads patients to need an ulnar shortening surgery where a piece of that bone is cut out. But what if this idea, that a long ulna causes this pain, was wrong? The patient would be exposed to a major and invasive surgery for no gain.
The Lowdown on Invasive Ulnar Shortening Surgery
This blog is meant as a companion blog to an earlier piece I did on why this surgery has no high-level evidence to support that it works and is loaded with complications. To read that first blog, click on its image below:

As a side note, I just performed an updated search on the research that supports this procedure. There is still not a single high-level study showing that it works or is even advisable.
Why Your Long Ulna Is Unlikely to Be Causing Pain
First, you need to understand that pain generation is a combination of three factors: structure, nerve irritation or damage, and the local chemical environment. Meaning, we have many, many studies showing that patients who seem to have structural abnormalities on X-rays or MRI that should be causing pain often have none. In addition, we have studies that show that patients with normal anatomy can be in severe pain. How is this possible? MRIs and X-rays don’t show the status of nerve irritation or the local chemicals that can lead to pain. So in many cases, while the anatomy is bad, the nerves are fine and the local chemicals are normal, hence, no pain. Or on the other side of that coin, the anatomy is fine, but the local nerves are irritated and are surrounded by toxic and inflammatory chemicals, so the patient hurts.
So right off the bat, you can see why any physician who understands this would be very wary of the idea that an X-ray showing a long ulna bone could ever make an accurate diagnosis of why someone has pain. It’s simply not enough information. So if this can’t be nailed as a cause, despite all of the surgeons wanting to cut off a chunk of your ulna, what might be the real cause? Let’s review a few.
Wrist Instability

Alila Medical Media/Shutterstock
One of the more common things I see in painful wrists is that they’re unstable. Meaning, at some point in someone’s life, a fall on an outstretched hand or catching a ball the wrong way stretched some of the many ligaments that hold the many wrist carpal bones in place (see pic to the left). This often goes unnoticed for many years while these bones move around too much. This extra motion causes wear and tear on the small joints, with pain and swelling. Since most doctors aren’t trained on how to find small amounts of instability, this often goes undiagnosed. In addition, an MRI is a static image (without movement), and this diagnosis can only be made when the wrist bones are moved. How is it usually fixed? Precise ultrasound-guided injections of platelet-rich plasma into the stretched ligaments to get them to heal and tighten down will usually provide stability.
Ulnar Nerve

Solar22/Shutterstock
The ulnar nerve supplies the ulnar (little-finger) side of the wrist. When it’s irritated anywhere along its course, pain in that outside wrist area can ensue. The nerve can get irritated as it passes through the elbow or shoulder. In the neck, this area on the hand is supplied by the C8 nerve, which can also be pinched. Through many years of nerve irritation, the structure can become scarred down, which makes things worse. Realize that you may feel no symptoms where the nerve is having problems, only in the wrist. Again, most doctors aren’t trained to find this kind of subtle nerve irritation nor is the usual MRI scan going to show it. How is it fixed? That depends on where the nerve is experiencing pressure. Sometimes physical therapy on the neck and shoulder will work; other times carefully injecting small amounts of platelet growth factors around the nerves using ultrasound imaging will do the trick. Other times the nerves in the neck may need to be injected using X-ray guidance.
TFCC
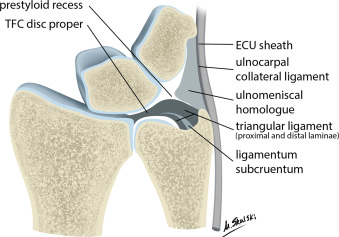
The TFCC is a triangular meniscus-shaped tissue on the ulnar side of the wrist that’s jacked into many small ligaments. It helps to cushion this side of the wrist and define motion. When this structure is injured, it’s often blamed on the long ulna bone, which is why surgeons want to cut. However, there are countless other things, like trauma, in someone’s distant past or wear and tear from repetitive movements that can cause damage or wear and tear to this ligament. We treat most of these injuries using a precise ultrasound-guided injection of either platelet-rich plasma or stem cells rather than surgery.
Tendonitis/Tenosynovitis
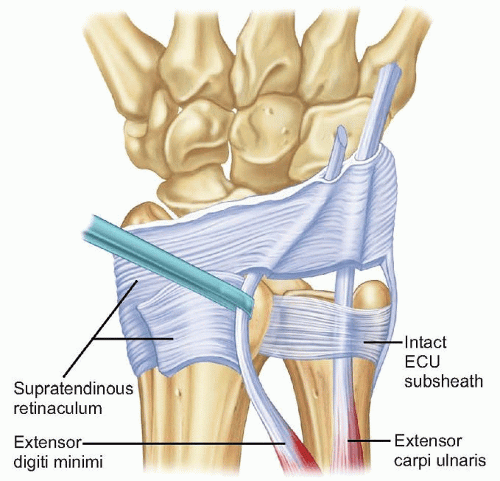
There are a few tendons at the side of the wrist that can also become damaged through old trauma or wear and tear. These tendons, when swollen, can cause pain. Again, this is often blamed on the long ulna bone, even though this is likely not the direct cause. So what can cause these tendons to become inflamed and be picked up on MRI? All of the items above, like an irritated nerve, an unstable wrist, or a TFCC problem. Fixing this issue usually involves two steps. Treatment for the cause and then the tendon. Precise platelet-rich injections using ultrasound guidance can help the damaged or worn tendons heal.
Why Do Famous Surgeons Want to Operate and How Could They Miss These Diagnoses?
Surgeons view the world in terms of surgery. Meaning their physical exam and review of imaging and history in a patient all revolves around whether there is a surgery that may help. In particular, because of the old adage if all you have is a hammer, everything looks like a nail, they commonly miss these other diagnoses. Interventional orthopedics is different. Here the treatments are broader and encompass a much wider number of diagnoses; hence, our job is to find this stuff that the surgeons miss and fix it without surgery. What is interventional orthopedics? See my video below:
The upshot? Please don’t let someone remove a piece of your ulna bone when there may be other wrist problems that have been missed and will go untreated. If you do end up with this extremely invasive surgery, make sure it’s only after all of the above have been ruled out or treated by an experienced interventional orthopedics physician.

NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.