Explore L5-S1 Disc Bulge Treatment Without Surgery

Medically Reviewed By:
An L5-S1 disc bulge can have a significant impact on daily life, often leading to pain, numbness, or weakness that makes routine activities challenging. Discomfort may extend to the lower back, hips, or legs, affecting mobility and overall function.
Surgery was previously considered the primary solution for addressing L5-S1 disc bulges. However, advancements in medical approaches have introduced non-surgical options that may help reduce pain and improve function.
What To Know About Spinal Discs And The L5-S1 Segment
Spinal discs serve as natural shock absorbers, cushioning the vertebrae and supporting movement. Each disc consists of two primary components: the nucleus pulposus, a gel-like inner core, and the annulus fibrosus, a tough outer layer. Together, these structures help maintain spinal flexibility and stability.

The L5-S1 segment is where the lumbar spine meets the sacrum at the base of the spine. This area supports a significant portion of the body’s weight and endures substantial stress, making it more prone to disc bulges and related issues. When the L5-S1 disc is affected, it may contribute to pain, stiffness, or nerve-related symptoms that impact mobility and function.
How L5-S1 Disc Bulge Affects The Spine And Nerves
An L5-S1 disc bulge occurs when the disc extends beyond its normal position, potentially pressing on nearby nerves. This pressure can affect the sciatic nerve, leading to weakness, tingling, numbness, or pain in the lower back, hips, legs, or feet.
In addition to nerve-related discomfort, a disc bulge may also limit spinal mobility, making bending or twisting more difficult. Depending on the severity and nerve involvement, symptoms can range from mild irritation to substantial pain, affecting daily activities and overall function.
Herniated vs. Bulging Discs
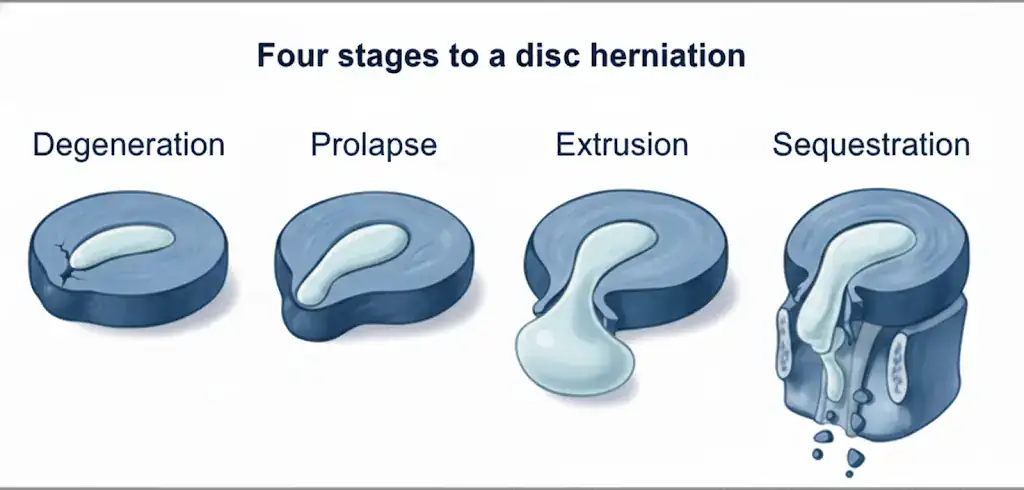
A herniated disc happens when the nucleus pulposus pushes through a complete tear in the annulus fibrosus. This is also known as an extruded disc. A bulging disc, on the other hand, occurs when the outer layer remains partially intact but weakens, causing the inner gel to push outward without fully escaping. This is known as a prolapsed disc.
Both conditions can put pressure on nearby nerves, potentially leading to back pain, numbness, tingling, burning sensations, or radiating discomfort in one or both legs. Since the L5-S1 disc is located at the base of the lumbar spine and bears significant weight and stress, it is particularly susceptible to these disc issues.
Surgical Solutions For Disc-Related Conditions
Physicians generally only recommend surgery when severe pain, loss of function, or nerve-related symptoms persist despite non-surgical treatments. These options aim to relieve pressure on nerves, restore mobility, and address structural issues caused by a disc bulge.
- Discectomy: Removes part or all of a damaged disc to reduce nerve compression, which may help alleviate pain and improve mobility. Unfortunately, this results in the removal of disc material and may leave a hole leaving the patient more susceptible for further disc bulges and herniations.
- Laminectomy: Involves removing the lamina (a part of the vertebra) to create more space for the spinal cord and nerves, potentially easing pressure and discomfort. This results in increased spinal instability and puts more stress on the nearby facet joints, which could contribute to degeneration over time.
- Artificial disc replacement: Replaces a damaged disc with an artificial one, aiming to maintain spinal movement while addressing pain. Unfortunately, research has shown that about 1 out of 10 patients with disc replacements fail and require surgical revisions within 1-2 years. This also carries a slight increase in the risk of degeneration in nearby spinal segments.
- Spinal fusion: Permanently joins two or more vertebrae to stabilize the spine, limiting movement in the affected area to reduce pain caused by instability. This increases pressure on nearby spinal segments, which increases the risk of developing degeneration over time.
- Laminoplasty: Re-shapes the lamina to relieve spinal stenosis, decompressing the spinal cord while preserving spinal movement.
- Foraminotomy: Expands the foramen (the boney opening where nerves exit the spine) by removing tissue or bone to alleviate nerve compression and associated symptoms. While small, this procedure carries a risk of nerve damage.
Potential Risks And Complications To Consider
While surgery may be an option for severe L5-S1 disc bulges, it is vital to understand the general risks and complications associated with spinal procedures. Understanding these factors can help individuals make informed decisions:
- Infection: Surgery carries a risk of infection at the surgical site or deeper in the spine, which may lead to increased pain, delayed healing, or additional interventions.
- Anesthesia Risks: Complications related to anesthesia can occur, particularly in individuals with underlying health conditions, including allergic reactions, breathing difficulties, low blood pressure, or heart-related issues.
- Recovery Time And Limitations: Recovery can take weeks to months, and movement may be restricted. Rehabilitation, including physical therapy, is often necessary to restore function, and some patients may require ongoing pain management.
- Need For Follow-up Care: Additional medical attention may be required if complications arise during recovery, though procedure-specific risks are addressed above.
How To Address L5-S1 Disc Issues While Avoiding Surgery
An L5-S1 disc bulge can often be managed through non-surgical means, depending on the symptom severity and individual health factors. Non-surgical treatments focus on approaches that may help reduce pain and may improve mobility, supporting the body’s natural healing process. Options include physical therapy, targeted exercise, medications, lifestyle factors, and interventional orthopedics procedures using Regenexx processing. These procedures may help address the underlying causes of discomfort and improve function without the risks and complications of surgery.
Some patients experience relief, while others with more severe conditions may require ongoing management or additional interventions. Non-surgical approaches are often considered before exploring surgical treatments.
Pain Management Techniques
Pain management techniques can help reduce discomfort and improve daily function for individuals with an L5-S1 disc bulge. Various non-surgical options focus on relieving symptoms and supporting overall spine health.
- Medications: Oral pain relievers or anti-inflammatory drugs may help manage discomfort and reduce inflammation.
- Topical treatments: Creams, gels, or patches applied to the affected area can provide localized relief.
- Heat/Cold therapy: Applying heat or cold can help relax muscles, reduce inflammation, and temporarily ease pain.
Physical Therapy
Physical therapy can help strengthen the muscles supporting the spine, improving posture, and enhancing flexibility. Targeted exercises may help alleviate pain, reduce pressure on the affected disc, and promote better spinal alignment.
Chiropractic Care
Chiropractic care focuses on spinal adjustments that may help improve alignment, reduce nerve pressure, and enhance mobility. Chiropractors use various techniques to manipulate the spine, which some individuals find beneficial for managing discomfort associated with an L5-S1 disc bulge. This approach may also support flexibility and overall spinal function.
Lifestyle Modifications
Making certain lifestyle adjustments can help reduce stress on the spine and support overall spinal health. Maintaining a healthy weight, practicing proper posture, and avoiding heavy lifting may help minimize strain on the L5-S1 disc and prevent further discomfort.
Engaging in low-impact exercises such as swimming, walking, or yoga can improve strength and flexibility, providing better support for the spine. Incorporating these habits into daily life may improve mobility and long-term relief.
Spine Conditions That May Benefit From Non-Surgical Approaches
The following spine conditions are commonly evaluated for non-surgical approaches, with treatments focused on managing symptoms and supporting overall spinal health.
The Regenexx Approach For Spinal Disc Issues
Physicians in the licensed Regenexx network use image-guided interventional orthobiologic procedures to treat disc-related conditions, including L5-S1 disc bulges. These non-surgical procedures are designed to support the body’s natural healing process and may help improve function and reduce pain.
Regenexx has developed proprietary lab processing and injection protocols that allow for precise delivery of orthobiologic materials to targeted areas of the spine.
The video below explains how orthobiologics work, outlines Regenexx procedures for disc injuries, and shares before-and-after MRI images.
Results vary. MRI changes do not guarantee pain relief or improved function.
Results vary. MRI changes do not guarantee pain relief or functional improvement.
Regenexx injectates for disc issues include:
Regenexx SCP Injectate
Regenexx SCP injectate uses a high concentration of platelets derived from the patient’s own blood. These platelets contain growth factors that may help reduce pain and may promote healing in the affected disc. This approach may help improve comfort and regain function, offering a potential option less invasive than surgery.
Regenexx SD Injectate
Regenexx SD injectate uses bone marrow concentrate, which contains healing agents, to address disc bulges. This procedure uses advanced imaging guidance to help achieve accurate placement in the affected area.
Case Study: Adam’s Recovery Journey With The Regenexx Approach
Adam first sought treatment in 2017 due to low back pain that had been gradually worsening since the previous summer. He had tried various treatments but had not experienced lasting improvement. He was looking for a non-surgical option for his L5-S1 disc bulge but had limited success with prior care.
Before considering procedures using Regenexx lab processes, Adam underwent an ultrasound-guided epidural with exosome-based injectates. While this initially provided some relief, his symptoms returned. He also tried acupuncture, deep tissue massage, chiropractic adjustments, and PRP injections with amniotic fluid, but none led to sustained improvement.
Adam reported experiencing discomfort when standing, bending, or reaching, as well as cramping and radiating pain in his hamstring after prolonged sitting. One factor contributing to his lack of progress may have been the placement of previous injectates. Precise placement between the disc and the affected nerve is critical, which requires imaging guidance beyond ultrasound.
A physician in the licensed Regenexx network took a different approach. Adam received two injections: one transforaminally using X-ray guidance and another infra-neural, targeting the nerve-disc interface. Growth factors from Adam’s own platelets were used, and additional affected structures were also treated.
Adam continued follow-up care for his L5-S1 disc condition and reported improvements in his symptoms over time. He was able to gradually return to a more active lifestyle and later opted for an additional procedure to support his ongoing recovery
This case highlights the importance of both precise injection placement and an individualized approach. With nearly two decades of experience, physicians in the licensed Regenexx network specialize in interventional orthobiologic procedures designed to help patients improve function and reduce pain.
Manage Discomfort With Spinal Health-Focused Approaches
Effectively managing discomfort from spinal conditions, such as an L5-S1 disc bulge, requires a comprehensive approach that prioritizes spinal health and overall well-being. Non-surgical options, including physical therapy, chiropractic care, and lifestyle modifications, may help reduce pain and improve mobility.
By exploring the right treatment strategies, individuals can take proactive steps to manage symptoms and enhance their quality of life while potentially avoiding invasive procedures. Physicians in the licensed Regenexx network offer interventional orthobiologic procedures designed to support spinal function and provide a non-surgical path to relief.
Get started to see if you are a Regenexx candidate
To talk one-on-one with one of our team members about how the Regenexx approach may be able to help your orthopedic pain or injury, please complete the form below and we will be in touch with you within the next business day.
Medically Reviewed By: