Stem Cell Disc Injection: The Hammer and the Nail
There’s a saying in medicine, “When all you have is a hammer, everything looks like a nail”. Meaning that if all the doctor knows how to do for a given problem is one treatment, then he or she tends to use that treatment when it’s not appropriate. This morning I’d like to highlight a stem cell disc injection that went wrong that explains why I’ve said that injecting stem cells into discs should only be reserved for specific patients and not everyone with back pain.
The Four Types of Low Back Disc Issues
Most patients don’t understand that all low back disc issues aren’t the same. First, it helps to understand that your low back discs are shock absorbers for the low back spine bones called vertebrae. They’re made up of a tough outer covering called the annulus and an inner gel called the nucleus. There’s much that can go wrong with both structures, which is why there are a few different types of injury.

The image above (click on it to see a bigger PDF) shows the four different disc damage types. Given that we have the world’s longest stem cell disc injection experience at 11 years, we’ve only found two disc types where this therapy is helpful. For same day stem cell treatments, a torn and painful disc that still has good height is almost a slam dunk in reducing the pain. For a very specially cultured type of stem cell disc injection (only available in Grand Cayman), a bulging disc pressing on a nerve can usually be made smaller. The other disc injury types including a collapsed disc and a herniated disc don’t respond to stem cells. To learn more about the different types of disc problems, click here.
Keeping Patients Safe is All About Applying the Least Invasive Therapy that’s Likely to Work
All too often in medicine, the hammer adage noted above gets applied and patients skip over much less invasive treatments and get offered much more invasive care. However, this is the opposite of what should happen, as this maximizes rather than minimizes risk.
If we apply this principle to someone with back pain, short of surgery, injecting something into the disc is the most invasive thing that can be done with a needle. Why? First and foremost, a disc infection (known as discitis) is awful. It means that the patient may need surgery to remove the infected disc and that the patient needs to be on IV antibiotics with a catheter inserted near the heart. Second, the doctor can damage the disc by injecting it, causing it to rapidly degenerate or herniate. More on this issue below.
What else could be done for back pain outside of injecting the disc? We successfully treat many back pain patients using advanced biologics like our third generation platelet rich plasma and our fourth generation platelet lysate without ever entering the disc. This is because we can use these substances epidural (around the nerves), in ligaments (to help tighten a loose degenerative spine), in atrophied stabilizing muscles (like multifidus), and in other joints like the facet or SI that may also be causing pain. Stem cells can also be injected into many of these same structures. Below is a video from April’s AAOM conference where I discuss the use of epidural platelet lysate to treat back pain.
A Low Back Disc Injection Gone Bad
Yesterday, one of our physician partners in our Colorado clinic came to me with the story of a patient who had received a disc injection at another local clinic and as a result had gotten much worse. While this can happen in any patient on any given day with any treatment, what was astounding was the fact that a totally normal appearing disc on MRI before the treatment had become quickly degenerated after the injection.
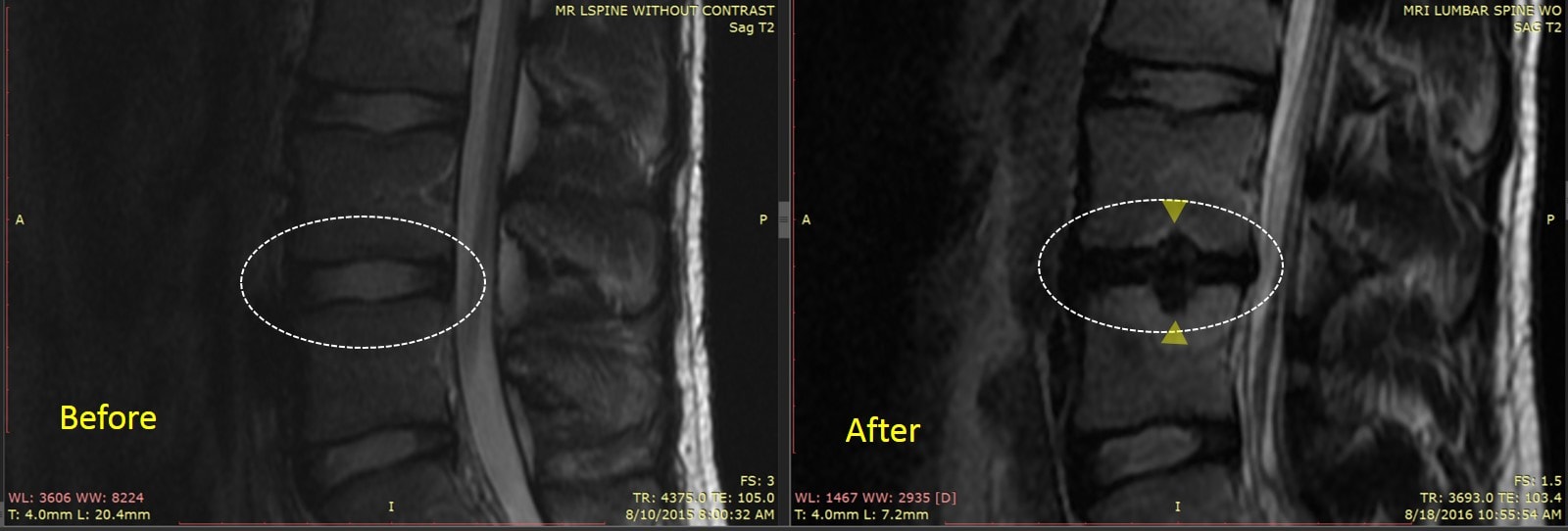
Note the patients MRI above from before the procedure. The disc inside the dashed circle had good height and is bright, which means it holds onto water well and is likely a good shock absorber. However, after the stem cell disc injection there are some “not so good” changes. The disc is now bulging and dark-meaning that it no longer has the ability to hold onto water and may irritate exiting nerves. The end plates (the top and bottom bony borders of the disc with the vertebra above and below), now have gaps in them known as Schmorl’s nodes (yellow triangles). So what appears to have been a normal healthy disc before the stem cell disc injection on the left is now a damaged looking disc on the right.
So what was wrong with this disc before the injection? Not much. No matter which slice I looked at of the MRI taken before the procedure, the disc looked normal. The patient also had the disc below at L5-S1 injected and it doesn’t seemed to have changed much. While this patient hadn’t done well with epidural steroid injections before the stem cell disc injection, since the surgeon who did the injection doesn’t have the ability to use platelet lysate epidural, we’ll never know if this patient would have responded to less invasive biologic therapies.
The upshot? While any patient at any time can get worse with any treatment, the best way to keep patients safe is to apply the least invasive treatment that might help. The problem right now is that most clinics offering to treat back pain with stem cells are one trick ponies – they only know how to inject stem cells into the disc in the most rudimentary way. They don’t know how to use less invasive platelet or stem cell based care outside the disc, where it may relieve back pain without placing the disc at risk for a complication. So again, caveat emptor…

NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.