We always need more PRP research. The problem becomes when what’s published is not accurate beginning with the title. Given that most doctors never read beyond the title and a few bullet points, that’s a problem. So let’s dive into a British study on Achilles tendinopathy and PRP that has lots of problems.
The British Achilles Study
The study was published in a major journal (JAMA), which makes this review all the more critical and their acceptance of this paper all the more comical. The title is “Effect of Platelet-Rich Plasma Injection vs Sham Injection on Tendon Dysfunction in Patients With Chronic Midportion Achilles Tendinopathy: A Randomized Clinical Trial” (7). This was a single-blinded study (the patient didn’t know which treatment they got) in patients with Achilles tendon pain for more than 3 months. One group got leukocyte-rich PRP and the other had dry needling. After 6-months, there was no difference in outcome between the groups.
Learn More About The Regenexx® Approach
Request a digital booklet and more information to learn about alternatives to orthopedic surgery and the Regenexx provider patient experience.
We do not sell, or share your information to third party vendors. By submitting the form you agree that you've read and consent to our Privacy Policy.
Concentration
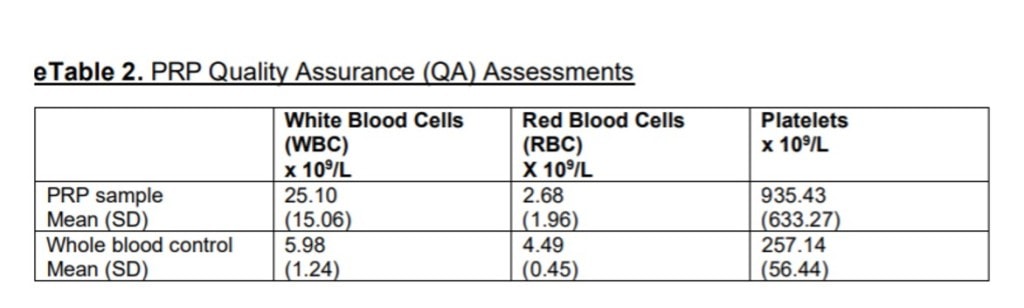
The PRP kits used were supposed to concentrate PRP to 8X over baseline. However, as shown above, it only concentrated the platelets 3-4 times over baseline. Why is this critical? The average age of the patients was 52 years old. Why does that matter?
Our tenocyte PRP study was published a few years back to determine what the effects of different concentrations were on young versus old tenocytes (1). What did we find? Older tenocytes (the cells being acted on by the PRP in this study) require much higher doses of PRP to facilitate healing. In fact, unlike in younger tendon cells, older cells have a direct dose dependant response to PRP. Meaning the higher the dose, all the way up to 14 times baseline (see image above), the better the tenocytes can bridge a gap and act. Hence, these Achilles tendons were clearly under-dosed based on our data. How low was the dose? Based on the data above, they got about half of the possible healing effect.
Red PRP
There are two main PRP types in use today. They look red and amber but have other differences. The red stuff is called “Leukocyte Rich (LR)” while the amber stuff is called “Leukocyte Poor (LP)”. LR has lots of red and white blood cells and LP has very few. They both have concentrated platelets.
The word on the street (meaning what physicians observe) is that red PRP causes way more inflammation, which makes sense as it contains white blood cells which mediate the inflammatory response. This has been borne out in experimental studies (2).
Looking at the table (eTable 2) I posted above it’s also critical to see what’s going on with WBCs (leukocytes) in the PRP used in this study. The leukocytes were concentrated on average 4.2 times over baseline while the platelets were concentrated only 3.6 times! So you really can’t call what they used platelet-rich plasma, but instead leukocyte-rich plasma with concentrated platelets!
Injection Technique
This was a blind 10-second injection into five spots with the leukocyte-rich plasma or a single injection under the skin. Note to all orthopedic surgeons, not using guidance to inject the Achilles tendon is BELOW the prevailing standard of care in 2021. Meaning for ours and many other clinics, it takes 10-15 minutes to properly inject an Achilles tendon using ultrasound guidance, making sure that all parts of the tendon are injected and that the more friable parties of the tendon are properly fenestrated. So whatever was done here was not at that same standard but BELOW the prevailing standard of care in use by experts in this field.
On the other side of the study, without guidance, how were the authors sure they were placing the sham needle just below the skin as described? Without using ultrasound, they couldn’t see where the needle was going. Why does it matter? Because as the authors brought up in the paper, dry needling is a treatment and not a placebo. Here are 4 randomized controlled trials showing that dry needling is effective in many musculoskeletal conditions including tendinopathy (3-6).
Even if they didn’t needle the tendon, how did they know that they didn’t enter the tendon sheath causing bleeding (again a treatment). Again, they don’t know because they didn’t use guidance. Given that the difference between being under the skin and in the Achilles tendon sheath is a millimeter (unless these physicians have magic hands), they likely entered the tendon sheath in some patients.
Incomplete Treatment
In our practice, Achilles tendinopathy is frequently comorbid with S1 radiculopathy. Meaning that an irritated S1 nerve in the low back is what causes the calf muscle to misfire and this beats up the Achilles tendon. So if you view the Achilles tendon in isolation, you are definitely less likely to help somebody’s pain. However, if you treat the back issue and the ankle issue together, you’re more likely to be successful.
The upshot? What should this title have been? “Effect of LEUKOCYTE-Rich Plasma and LOW DOSE PLATELETS BLIND Injection vs Sham Injection? (WE’RE NOT SURE) on Tendon Dysfunction in Patients With Chronic Midportion Achilles Tendinopathy: A Randomized Clinical Trial”. Meaning this wasn’t PRP, it likely had too few platelets to show an effect, this was a below standard of care blind injection, and it’s comical that JAMA couldn’t string together enough reviewers who understood the field to review the paper.
__________________________________________
References:
(1) Berger DR, Centeno CJ, Steinmetz NJ. Platelet lysates from aged donors promote human tenocyte proliferation and migration in a concentration-dependent manner. Bone Joint Res. 2019 Feb 2;8(1):32-40. doi: 10.1302/2046-3758.81.BJR-2018-0164.R1. PMID: 30800297; PMCID: PMC6359887.
(2) Anitua E, Zalduendo M, Troya M, Padilla S, Orive G. Leukocyte inclusion within a platelet rich plasma-derived fibrin scaffold stimulates a more pro-inflammatory environment and alters fibrin properties. PLoS One. 2015 Mar 30;10(3):e0121713. doi: 10.1371/journal.pone.0121713. PMID: 25823008; PMCID: PMC4379078.
(3) Pai MYB, Toma JT, Kaziyama HHS, Listik C, Galhardoni R, Yeng LT, Teixeira MJ, Ciampi de Andrade D. Dry needling has lasting analgesic effect in shoulder pain: a double-blind, sham-controlled trial. Pain Rep. 2021 Jun 28;6(2):e939. doi: 10.1097/PR9.0000000000000939. PMID: 34235343; PMCID: PMC8240781.
(4) Kheradmandi A, Kamali F, Ebrahimian M, Abbasi L. Comparison between dry needling plus manual therapy with manual therapy alone on pain and function in overhead athletes with scapular dyskinesia: A randomized clinical trial. J Bodyw Mov Ther. 2021 Apr;26:339-346. doi: 10.1016/j.jbmt.2020.11.017. Epub 2020 Nov 24. PMID: 33992267.
(5) Sánchez-Infante J, Bravo-Sánchez A, Jiménez F, Abián-Vicén J. Effects of Dry Needling on Muscle Stiffness in Latent Myofascial Trigger Points: A Randomized Controlled Trial. J Pain. 2021 Jul;22(7):817-825. doi: 10.1016/j.jpain.2021.02.004. Epub 2021 Feb 23. PMID: 33636373.
(6) Ceballos-Laita L, Jiménez-Del-Barrio S, Marín-Zurdo J, Moreno-Calvo A, Marín-Boné J, Albarova-Corral MI, Estébanez-de-Miguel E. Effectiveness of Dry Needling Therapy on Pain, Hip Muscle Strength, and Physical Function in Patients With Hip Osteoarthritis: A Randomized Controlled Trial. Arch Phys Med Rehabil. 2021 May;102(5):959-966. doi: 10.1016/j.apmr.2021.01.077. Epub 2021 Feb 7. PMID: 33567336.
(7) Kearney RS, Ji C, Warwick J, Parsons N, Brown J, Harrison P, Young J, Costa ML; ATM Trial Collaborators. Effect of Platelet-Rich Plasma Injection vs Sham Injection on Tendon Dysfunction in Patients With Chronic Midportion Achilles Tendinopathy: A Randomized Clinical Trial. JAMA. 2021 Jul 13;326(2):137-144. doi: 10.1001/jama.2021.6986. PMID: 34255009.
Chris Centeno, MD is a specialist in regenerative medicine and the new field of Interventional Orthopedics. Centeno pioneered orthopedic stem cell procedures in 2005 and is responsible for a large amount of the published research on stem cell use for orthopedic applications. View Profile
NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.