Why is the Thoracic Spine a No Man’s Land?

Credit: Shutterstock
A patient came in recently to discuss the effects of PRP treatment she received in Canada. Out of that conversation came a common refrain. A Toronto spine specialist didn’t want to repeat her prior very successful thoracic spine interventional treatment that I had done in Colorado. Why? He had never treated this area of the spine before and wasn’t comfortable with it. This brings up a big issue that’s worthy of discussion. Why is the thoracic spine a not uncommon pain generator and yet so often ignored by even experienced interventional spine physicians? Let’s dig in.
The Thoracic Spine
The thoracic spine is numbered T1-T12 and is located between your neck and low back. This is where your ribs attach. It has discs, facet joints, and nerves just like the rest of your spine. It also has added joints and ligaments between the ribs and spinal bones.
Thoracic Pain
The thoracic spine has lots of structures that cause pain:
Thoracic Facet Joints

Adapted from Bogduk et al
There are facet joints in the thoracic spine where the vertebra above and below articulate. They can refer pain to the adjoining areas, just like there are facet joints in the neck that do the same (see above). These facet joints act just as they do in other parts of the spine, as finger-sized joints that help control motion. They can be injured or get arthritis.
Rib Facet Joints
Young, B.A., Gill, H.E., Wainner, R.S. et al. Thoracic costotransverse joint pain patterns: a study in normal volunteers. BMC Musculoskelet Disord 9, 140 (2008). https://doi.org/10.1186/1471-2474-9-140
The ribs attach to each vertebra at two points-one costotransverse and one costovertebral joint. They are attached with strong ligaments that help to control rib motion, and each of these joints, when damaged, can refer pain to other areas, as shown above.
Thoracic Disc Bulges and/or Herniations

The discs in the thoracic spine can bulge out just like those in the neck and low back. When that happens, they can irritate thoracic spinal nerve roots, which have dermatomal patterns just like other spinal nerves (shown above). This can cause radiating pain that wraps around the ribs goes into the chest or stomach or just lives in the upper back. There may also be numbness/tingling, or burning.
Each level in the thoracic spine also has a disc, just like in other areas of the spine. These can bulge and irritate nerve roots as well as produce pain all on their own through annular tears.
Scapulothroacic Bursa
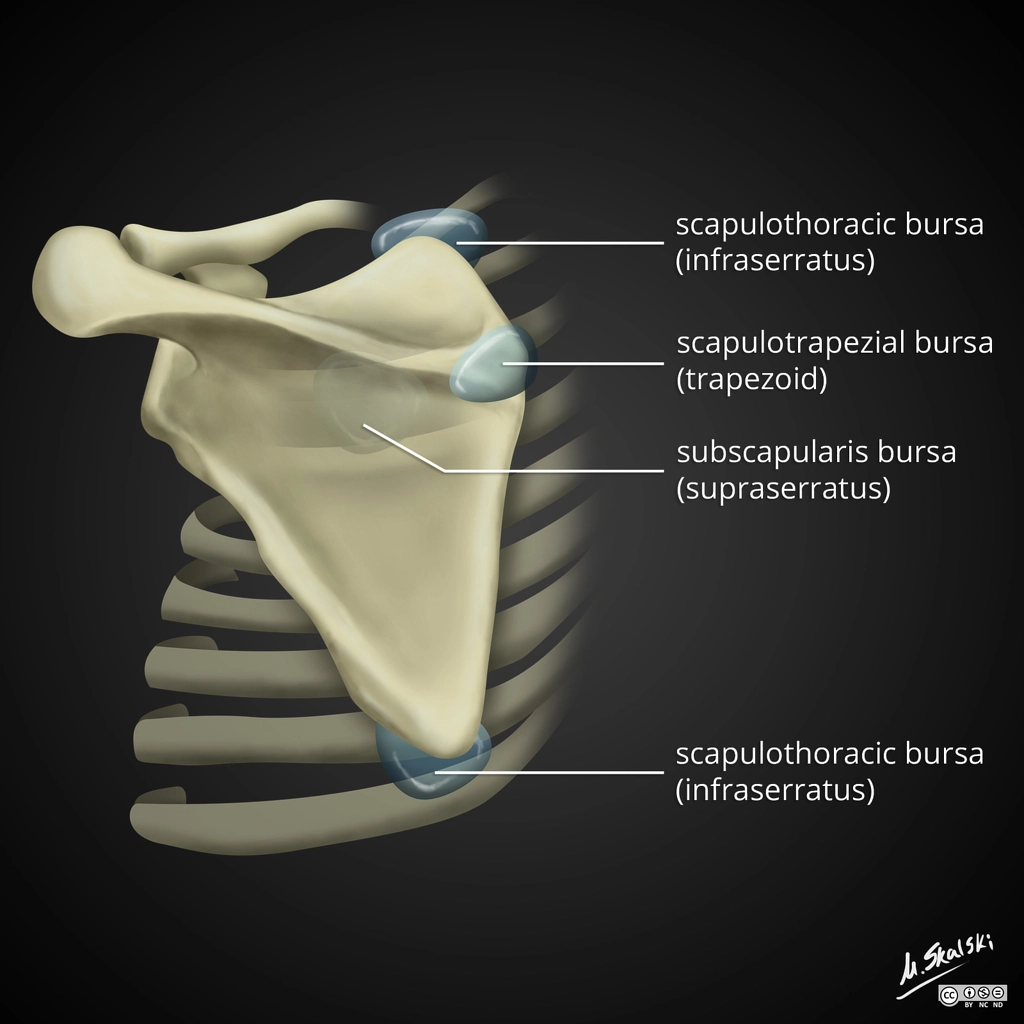
Credit: Radiopedia
There are lubricating sacs (bursae) between the scapula and the ribs and various connecting muscles. These can become inflamed due to abnormal scapular motion or abnormal underlying rib motion and can cause pain.
Muscles and Tendons
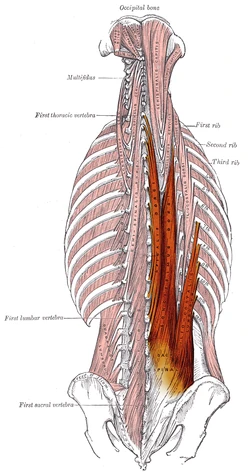
Credit: Wikipedia Commons
There are many muscles in the thoracic spine. One of the frequent areas we see problems develop is in the tendons that attach to the ribs (as shown above). This type of tendinopathy tends to happen in patients with low back problems that cause the deep lumbar multifidus to go offline, forcing these thoracic muscles to overwork to compensate.
Rib Fascia
The rib cage is surrounded by the fascia. What’s that? If you’ve ever eaten the dish called “ribs” you know that there is a tough layer of connective tissue around those bones, and this is called the fascia. It helps to shape and control rib motion. When it gets injured or stretched out, abnormal rib motion can occur, leading to ribs “popping put” or a sensation that a rib is out of place. This pain is usually made worse by taking a deep breath, and chiropractic or other types of manipulation can frequently help.
Why is Treatment in the Thoracic Spine So Rare?
To illustrate this point, a patient about five years ago came in with disabling stomach pain. His doctors at the local university eventually realized that it had something to do with his spine, but nobody there wanted to inject his thoracic spine, which was the real cause. Instead, they gave him fluoroscopically guided upper lumbar injections, which didn’t work. The pain was so severe that he was considering suicide and he had a plan to kill himself. A simple lower thoracic epidural and treating the rib fascia with PRP were all he needed to have the problem solved. He obviously never committed suicide. Why did this happen?
The thoracic spine is surrounded by the rib cage and lungs. Hence, any injection needs to take into account avoiding the lung field. The same with surgeries, where oftentimes the lung needs to be deflated and the patient placed in the ICU as part of the surgery. All of this takes additional technical expertise. Because of this fact, there is substantial institutional momentum built up against injecting or operating on the thoracic spine. When it comes to fluoroscopy-guided spine injections, that means the epidural area, facets, ligaments, muscle tendons, and discs rarely get treated. Add in that some of these injections, like injecting thoracic facets, are much more time intensive than injecting the same structures in the neck and low back, and the thoracic spine is just crossed off the list as a treatment possibility.
What Should be in Your Doctor’s Tool Box for the Thoracic Spine?
First, our clinic abandoned high-dose steroid injections in the spine many years ago due to their serious side effects. Hence, everything I’ll talk about here is either platelet or bone marrow concentrate based care. Here’s a list of thoracic injection procedures we frequently use at our Colorado Regenexx HQ site:
- Thoracic facet injection with fluoroscopy
- Rib facet joints or ligaments using either fluoroscopy or ultrasound
- Thoracic transforaminal epidural injection with fluoroscopy
- Thoracic Disc Injection with fluoroscopy
- Ultrasound-guided scapular bursa injections
- Ultrasound-guided tendon injections
- Ultrasound-guided rib fascia injections
How Can You Get Thoracic Treatment?
This is the most difficult part, as educating patients on what might be wrong or what might help is easy, but finding an expert who knows how to diagnose and treat the thoracic spine is very hard for all of the reasons we discussed above. These experts are few and far between. This all begins with a good hands-on exam in this area. What does that look like?
First, the doctor needs to palpate your thoracic spine and ribs to find out what hurts. Second, a check of thoracic dermatomes (nerve root territories on the skin) needs to be done by using a Wartinburg wheel up and down the thoracic spine to find areas of decreased or increased sensation that might indicate if you have an irritated spinal nerve. Next, the movement and range of motion of the thoracic area should be accessed. Finally, the movement of the rib change while you breathe in and out should also be investigated, looking for injuries to the rib fascia.
There’s another part of the exam that’s critical, and that’s spending time reviewing your MRI images with you, looking for problems that correlate to your exam. This should include the following:
- Reviewing each disc level looking for the telltale signs of a disc bulge
- Observing each facet and rib facet joint
- Taking note of any multifidus atrophy (deep spinal stabilizer) that can indicate chronic spinal nerve irritation
An expert in the thoracic spine should NEVER rely solely on the MRI report!
What if you have chronic thoracic pain and you’ve never had this kind of thoracic exam? Find another doctor because the doctor you’re with isn’t an expert in this area.
The upshot? The thoracic spine shouldn’t be a no man’s land that the vast majority of spine experts skip over. It can produce pain just like the neck and the low back, and it can be treated with additional interventional expertise. However, finding a doctor who wants to dig in here and identify what’s wrong isn’t that easy.

NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.