ACL Tear Repair Without Surgery in New Jersey
Are You a Regenexx Candidate?Physicians in the licensed Regenexx network often address Anterior Cruciate Ligament (ACL) injuries, which are common knee conditions. While typical surgical intervention has long been the standard for complete ACL tears, newer, minimally invasive options using interventional orthobiologics are now available.
Procedures using Regenexx lab processes, such as Perc-ACLR (percutaneous ACL repair), may offer an alternative approach for treating certain ACL injuries. This approach utilizes your body’s own healing agents to support the natural repair process, potentially avoiding the need for surgery. In appropriate cases—especially those involving non-retracted partial or full tears—these procedures may help reduce pain and may improve joint stability.
Repair of ACL tear without surgery
ACL Tear Recovery Time Without Surgery
When evaluating options after an ACL injury, it is important to thoroughly weigh all treatment approaches, considering factors like the expected recovery timeline, potential return to activity, and the potential long-term impact on joint health.
Procedures using Regenexx injectates are developed to preserve the existing ACL structure whenever possible, rather than opting for removal or replacement.
Perc-ACLR is a procedure using Regenexx lab processes that utilizes image-guided delivery of the individual’s own bone marrow concentrate. This minimally invasive approach is typically completed in a single day. In appropriate cases, this option may support the body’s natural healing response and may offer a shorter recovery period compared to typical surgical intervention.
| Perc-ACLR | Surgery | |
|---|---|---|
| Procedure Invasiveness | Much less | Much more |
| Return to Sports | 3 to 6 months | 1 year |
| Keep your ACL | Yes | NO |
| Recovery | Brace, much less extensive PT | Crutches, brace, extensive PT |
345 State Street
Perth Amboy, NJ 08861
Request an Appointment
Call to Schedule Schedule OnlineClinic Hours
| Sunday | Closed |
| Monday | 9AM–5PM |
| Tuesday | 9AM–5PM |
| Wednesday | 9AM–5PM |
| Thursday | 9AM–5PM |
| Friday | 9AM–5PM |
| Saturday | Closed |
How Does the Regenexx Approach Work?
The Regenexx approach uses interventional orthobiologics, a specialized form of orthopedic care. This approach was developed as a minimally invasive alternative to typical ACL surgery.
These procedures utilize advanced image-guidance, such as ultrasound or fluoroscopy, to ensure the precise delivery of the individual’s own bone marrow concentrate directly to the injury site within the knee joint. The healing agents present in the bone marrow concentrate may help support the body’s natural healing response. In appropriate cases, this method may assist patients with certain ACL tears, potentially avoiding the need for surgical intervention[1].
Regenexx for ACL Tears: Perc-ACLR
Available at Pain Doctors Medical – Perth Amboy, New Jersey
The Perc-ACLR procedure, which uses Regenexx injectates and lab processes, may offer a minimally invasive alternative to typical ACL surgery. This treatment option is often completed over the course of a single day.
The process begins with the extraction of a small amount of the individual’s bone marrow. A physician in the licensed Regenexx network performs this using precise imaging guidance and specialized techniques licensed by Regenexx. Next, the drawn bone marrow is processed by a trained lab technician following proprietary Regenexx protocols. Following processing, patients typically have a rest period before the physician performs the reinjection, which generally occurs approximately three to six hours later.
The physician uses advanced imaging, such as fluoroscopy (real-time X-ray guidance) and MRI imaging with contrast, to create a thorough map of the ACL tear. This roadmap helps guide the physician in precisely placing the processed bone marrow concentrate into the affected areas of the ligament. Local anesthesia is applied to enhance patient comfort during the reinjection.
Following the procedure, patients may experience mild joint soreness, which can last for one to three days, with general discomfort typically decreasing within five to seven days. Many individuals report functional improvement within a month. During early recovery, patients may begin physical therapy and light activity.
Note: Individual outcomes may vary. For more information about patient outcomes, please visit our Patients’ Results page: https://regenexx.com/results/.
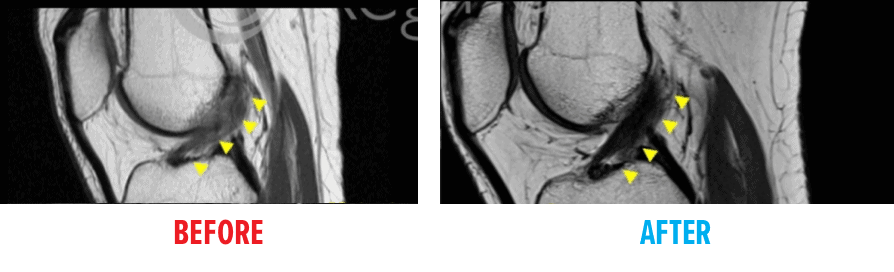
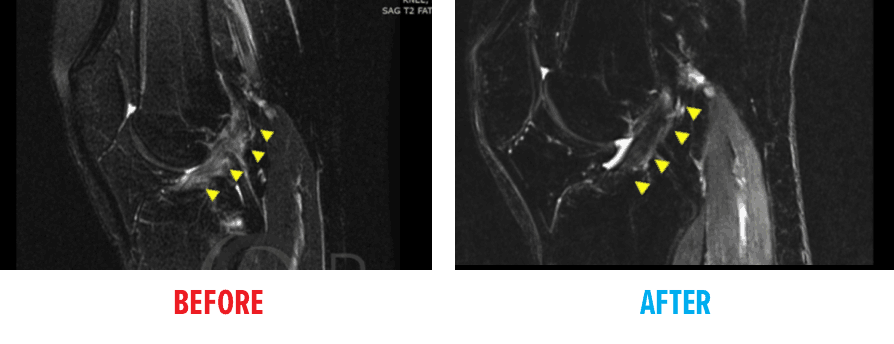
Before and After MRI Images
These MRI images visually demonstrate the structural changes noted in individuals who had procedures using Regenexx lab processes as a potential alternative to typical ACL surgery.
In the “before” image, the Anterior Cruciate Ligament (ACL) structure appears disrupted. Following the procedure, the “after” image shows a more continuous dark band running diagonally across the joint, which is an appearance often associated with a more intact ligament structure.
FAQs
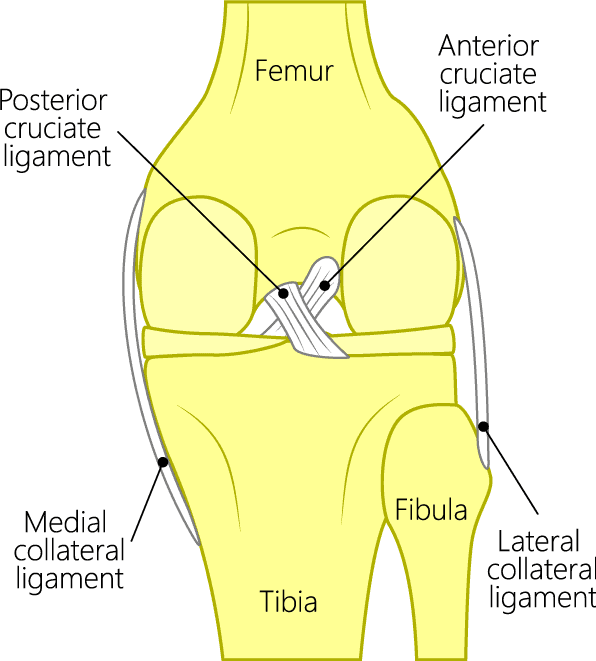
Knee joint anatomy showing ACL
There are two cruciate (meaning “cross-shape”) ligaments found inside your knee joint that work to stabilize it. They cross each other to form an X with the anterior cruciate ligament (ACL) in front and the posterior cruciate ligament (PCL) in the back. The ACL prevents the knee from sliding forward and the PCL from sliding backward.
ACL surgery is not generally an emergency procedure unless there is extensive damage to other structures, significant instability, or intense pain. Generally, if there is some joint stability, adults can delay surgery for a month or two. For young athletes, the waiting period may be slightly less and is often determined by a desire to get the injury repaired in the hope of returning to sports quickly. For some patients, delaying surgery and trying physical therapy first may help the healing process. If that fails, there are nonsurgical options, such as Perc-ACLR, to consider prior to resorting to surgery.
Research has also shown that ACL sprains and even complete ACL tears can regrow and heal on their own,2 particularly if interventional orthopedic procedures such as the Perc-ACLR procedure are utilized. These techniques do not require surgery and employ your body’s natural healing agents to repair your ACL injury. So, if your body can heal your ACL naturally, why would you choose surgery?
ACL sprains, tears, and ruptures are all essentially the same thing, and the terms are used interchangeably. Injured knee ligaments are all considered “sprains” and are graded on a severity scale.
- Grade 1 Sprains: The ligament is mildly damaged in a Grade 1 Sprain. It has been slightly stretched but is still able to help keep the knee joint stable.
- Grade 2 Sprains: A Grade 2 Sprain stretches or mildly tears the ligament to a point that the ACL becomes loose. This is also sometimes referred to as a partial tear of the ligament.
- Grade 3 Sprains: This type of sprain is most commonly referred to as a complete tear of the ligament. The ligament has been split into two pieces, and the knee joint is unstable.
An ACL rupture is another term often used to describe a tear. However, ruptures of the ACL are generally equated with complete full-thickness tears (Grade 3 Sprains) and are often associated with ligament deformity or full retraction.
Statistically, only about half of athletes who have ACL reconstruction regain complete function after rehab and are able to return to sport at the same level. The other half regain knee stability but not normal biomechanics or proprioception equal to the noninjured knee. Functional limitations in daily life are also possible. It is always advisable to get a second opinion on the need for surgery as there are a number of documented complications associated with conventional ACL reconstruction surgery and your injury could have been misdiagnosed. While surgery might be the right procedure for some ACL injuries, the vast majority of people could avoid it.
- Approximately 17 percent of adults will experience anterior knee pain or pain on kneeling, and between 5 percent and 29 percent will experience graft failure and loss of knee joint stability, with younger patients having higher rates. Other potential complications include knee stiffness or loss or range of motion (approximately 5 percent), painful hardware (approximately 6 percent), infection (approximately 1 percent to 2 percent) or patellar tendon rupture/patellar fracture in the case of bone-to-bone grafts.3-6
- Increased youth participation in high-intensity elite sports has resulted in much higher rates of ACL repair surgery in young teens, however, research is now suggesting that postsurgery complications may be worse in kids than adults. If preserving the natural physical gifts you were born with and “keeping original parts and structures intact” is your goal, you may want to consider a nonsurgical alternative like Perc-ACLR.
- A large analysis of 160 clinical trials demonstrated higher rates of postsurgery complications in young teens undergoing ACL repair and found that the risk for growth disturbances, skeletal deformities, and ligament rerupture requiring a second surgery was much higher in this young (average age = 13), skeletally immature population.7
- A 2010 Swedish research study also challenged the concept that surgery is the only way to heal ACL tears. They demonstrated that 60 percent of the athletes (average age = 26) who elected a strict physical therapy regimen over surgery never needed to have the ACL replaced and were still able to play sports.8
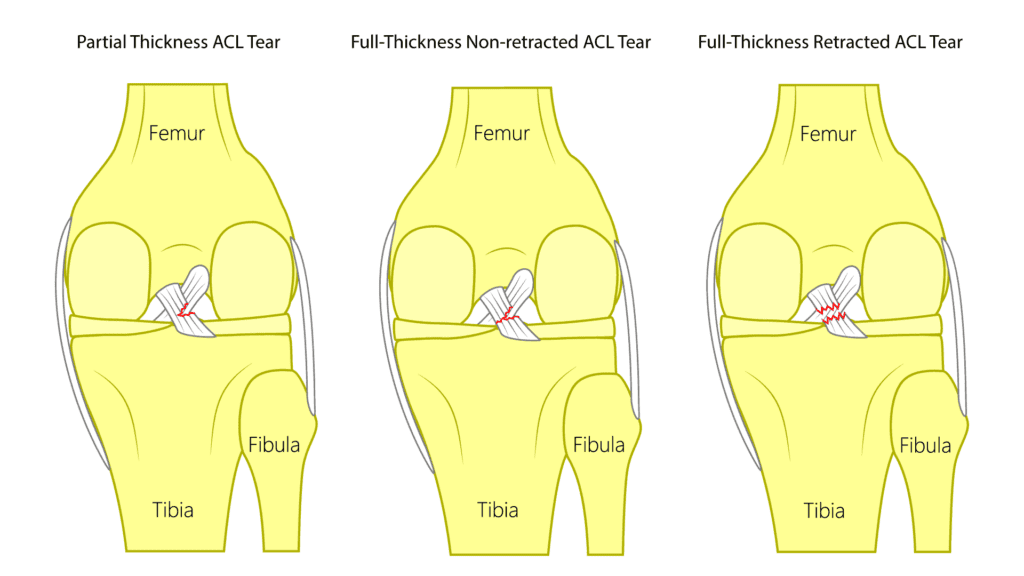
ACL tears can be classified in many ways, but within regenerative medicine, they are typically grouped into three primary types: partial-thickness, full-thickness non-retracted, and full-thickness retracted tears. Both partial-thickness and full-thickness non-retracted tears may be suitable for treatment using regenerative approaches such as the Regenexx knee Perc-ACL procedure, which promotes healing without the need for surgery. In contrast, full-thickness retracted tears usually require surgical repair to restore proper function.
- Partial-Thickness ACL Tear
A partial-thickness tear does not extend through the entire ligament. Imaging typically reveals that a portion of the ACL remains intact, indicating that the tear is incomplete. - Full-Thickness Non-Retracted ACL Tear
This type of tear involves a complete disruption of the ligament fibers; however, the torn ends have not separated significantly. The ligament is fully torn, but the pieces remain aligned and have not recoiled or retracted, making it potentially responsive to regenerative treatment. - Full-Thickness Retracted ACL Tear
In this case, the ligament has torn completely, and the ends have pulled apart—often recoiling like a stretched rubber band that snaps. This displacement generally limits the success of nonsurgical options and typically necessitates surgical reconstruction.
ACL tears
Get started to see if you are a Regenexx candidate
To talk one-on-one with one of our team members about how the Regenexx approach may be able to help your orthopedic pain or injury, please complete the form below and we will be in touch with you within the next business day.
References
1. Centeno C, Markle J, Dodson E, Stemper I, Williams C, Hyzy M, Ichim T, Freeman M. Symptomatic anterior cruciate ligament tears treated with percutaneous injection of autologous bone marrow concentrate and platelet products: a non-controlled registry study. J Transl Med. 2018 Sep 3;16(1):246. doi: 10.1186/s12967-018-1623-3. PMID: 30176875. PMID: 30176875. [Google Scholar]
2. Costa-Paz M, Ayerza MA, Tanoira I, Astoul J, Muscolo DL. Spontaneous healing in complete ACL ruptures: a clinical and MRI study. Clin Orthop Relat Res. 2012 Apr;470(4):979-85. doi: 10.1007/s11999-011-1933-8. PMID: 21643922. [Google Scholar]
3. Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR Jr. Arthroscopic anterior cruciate ligament reconstruction: a metaanalysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med. 2003 Jan-Feb;31(1):2-11. doi: 10.1177/03635465030310011501. PMID: 12531750. [Google Scholar]
4. Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. 2014 Mar;42(3):641-7. doi: 10.1177/0363546513517540. Epub 2014 Jan 22. PMID: 24451111. [Google Scholar]
5. Burks RT, Friederichs MG, Fink B, Luker MG, West HS, Greis PE. Treatment of postoperative anterior cruciate ligament infections with graft removal and early reimplantation. Am J Sports Med. 2003 May-Jun;31(3):414-8. doi: 10.1177/03635465030310031501. PMID: 12750136. [Google Scholar]
6. Kovacic JJ in Complications of Anterior Cruciate Ligament Surgery, AAOS Monograph Series 2005. Accessed August 25, 2020.
7. Wong SE, Feeley BT, Pandya NK. Complications After Pediatric ACL Reconstruction: A Meta-analysis. J Pediatr Orthop. 2019 Sep;39(8):e566-e571. doi: 10.1097/BPO.0000000000001075. PMID: 31393290. [Google Scholar]
8. Frobell RB, Roos EM, Roos HP, Ranstam J, Lohmander LS. A randomized trial of treatment for acute anterior cruciate ligament tears. N Engl J Med. 2010 Jul 22;363(4):331-42. doi: 10.1056/NEJMoa0907797. Erratum in: N Engl J Med. 2010 Aug 26;363(9):893. PMID: 20660401. [Google Scholar]