Non-Surgical Options for Managing Knee Osteoarthritis
Knee osteoarthritis (OA) stands as one of the most frequently diagnosed orthopedic conditions . For those experiencing this condition, the resulting discomfort may interfere with daily activities and affect overall well-being.
When individuals over 40 develop knee pain related to osteoarthritis—commonly termed arthritis—initial medical guidance typically suggests conservative measures. These approaches often involve physical therapy, nonsteroidal anti-inflammatory medications (NSAIDs), or injections of corticosteroid or hyaluronate to help manage inflammation and discomfort.
If these initial treatments fail to produce meaningful improvement, arthroscopic surgery may be considered to address damaged cartilage or tissue. Should symptoms continue even after these procedures, total knee replacement is often presented as the next course of action.
Alternative to knee replacement surgery for osteoarthritis
Can Knee Surgery Help Reduce Pain?
Numerous studies[2] evaluating the outcomes of typical orthopedic knee surgeries suggest that these procedures may offer limited benefit, especially for individuals over the age of 40. Even in younger patients, success is not universal. Some patients are unaware that surgery may not always be the most appropriate solution.
Read on to learn more about the Regenexx approach at Pain Doctors Medical, which offers an alternative to knee replacement surgery for osteoarthritis. These procedures utilize interventional orthobiologics to support the body’s natural healing response, and they may help reduce pain and improve function. Treatment is delivered by physicians in the licensed Regenexx network and is customized to individual needs.
345 State Street
Perth Amboy, NJ 08861
Request an Appointment
Call to Schedule Schedule OnlineClinic Hours
| Sunday | Closed |
| Monday | 9AM–5PM |
| Tuesday | 9AM–5PM |
| Wednesday | 9AM–5PM |
| Thursday | 9AM–5PM |
| Friday | 9AM–5PM |
| Saturday | Closed |
How Does the Regenexx Approach Work for Knee Osteoarthritis?
Physicians in the licensed Regenexx network at Pain Doctors Medical in Perth Amboy, New Jersey, utilize Regenexx procedures as part of an approach called interventional orthobiologics. This minimally invasive option compared to knee surgery uses image-guided injection of the individual’s own bone marrow concentrate directly into the joint.
The cellular elements in the concentrate may support the body’s natural healing response at the injury site and may help reduce the need for surgery.
The Regenexx Approach for Knee Arthritis
Physicians in the licensed Regenexx network conduct a thorough evaluation of movement patterns and may use ultrasound imaging to view the joint’s internal structures in real time . This approach provides a clearer understanding of the cause of pain, how joint function is impacted, and what underlying issues are contributing to the condition.
Following this evaluation, the physician will develop a customized treatment pla . Recommended procedures may utilize one or more of the following Regenexx injectates:
- Regenexx SD Injectate: A procedure using bone marrow concentrate, which contains cellular elements , prepared according to Regenexx intellectual property.
- Regenexx SCP Injectate: A proprietary formulation of platelet-rich plasma (PRP) that is more concentrated than PRP produced by typical bedside centrifuge devices.
- Regenexx PL Injectate: Platelet lysate (PL), a specialized derivative of platelet-rich plasma (PRP).
See how Regenexx helped Stephanie with her chronic pain from knee osteoarthritis.
Note: Like all medical procedures, Regenexx procedures have a success and failure rate. Not all patients will experience the same results.
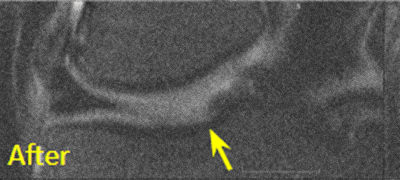
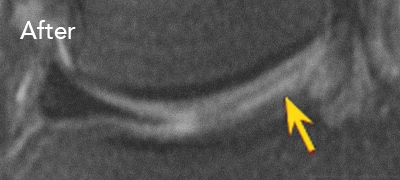
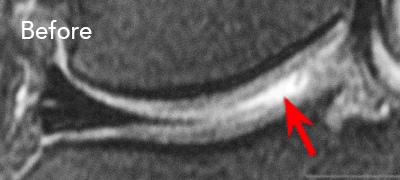
BEFORE and AFTER MRI Images
The MRI images provided below illustrate the changes observed in two individuals who underwent procedures using Regenexx lab processes for knee osteoarthritis.
To view the knee joint before the procedure, scroll the arrow to the right; the white or lighter areas within the joint space may visually indicate regions of joint degeneration. To view the MRI of the knee joint following the procedure, scroll the arrow to the left.

Patient 1:
This individual experienced limited improvement following a microfracture procedure and was unable to resume many daily activities. A procedure using a percutaneous injection of autologous cells processed using Regenexx lab methods was later performed. Following the procedure, the individual reported returning to routine functional activities.
Patient 2:
This individual underwent arthroscopic debridement, during which a 3 cm by 4 cm osteochondral defect on the medial femur was identified. Approximately 1.5 years after surgery, the individual received a percutaneous procedure involving autologous cells processed using Regenexx lab methods. Subsequent to the procedure, the individual reported resuming full functional activities.
Patient FAQs
The knee is actually a joint — the largest one in the body. It is where the thigh (femur) and shin bones (tibia and fibula) meet. The ends of our bones are covered in a smooth, slippery material known as cartilage that helps lubricate the knee joint. This allows the bones to move against each other without friction and protects your joint from stress. Your knee also has two rings of fibrous cartilage known as the meniscus. This structure helps provide stability to the joint and distribute weight evenly.
The knee joint experiences a significant load during weight-bearing activities over a person’s life span. All joints go through normal cycles of damage and repair that can involve thinning and damaging of cartilage, bone spurs, and more, but sometimes the body’s repair process results in changes to the shape or structure of the joints. When this happens, the bones of the joint may no longer be properly aligned or lubricated, which, over time, can cause inflammation, pain, swelling, and stiffness known as osteoarthritis. Osteoarthritis can be a result of being overweight, normal aging, or an injury to the joint.
Arthritis is a general term that describes joint inflammation. There are two types of arthritis
- Osteoarthritis (OA) – also called degenerative joint disease, is the most common type of arthritis and happens when the cartilage in your joints breaks down, often in your hips, knees, and spine.6
- Rheumatoid arthritis (RA) – is an autoimmune disorder where the immune system identifies the lining of the joints (synovium) as a threat and attacks it.7
Yes. When we have looked at our data, patients who had less severe arthritis did no better than patients who had bone-on-bone arthritis. Other data published by other authors also confirm this.8
Both X-rays and magnetic resonance imaging (MRI) can show degenerative arthritis changes in the joints. However, symptoms of osteoarthritis may arise before the damage can be seen in standard X-rays. So practitioners will often use the more sensitive magnetic resonance imaging, which is superior for detecting early osteoarthritis. Also, MRIs show three-dimensional images, while X-rays do not.
While cartilage is important for maximal functioning, its loss is not what causes pain. The most consistent MRI finding associated with pain is swelling in the bone called bone marrow edema (BME) or a bone marrow lesion (BML). Current research on knee pain due to arthritis has shifted from cartilage loss to this bone marrow swelling.
No, they won’t regrow large stretches of cartilage; however, they will help:
- Replace a worn-out stem cell reserve. The number of those cells available for repair and maintenance goes down as we age and get arthritis.
- Reboot dying stem cells. Studies have shown that mesenchymal stem cells can give their good batteries (mitochondria) to cells that have worn-out batteries, rebooting those dying cells.
- Treat bone lesions. Microfractures, not cartilage loss, are the source of pain.
- Reset the environment. The environment inside an arthritic joint has a mix of inflammatory and damaging chemicals.
Get started to see if you are a Regenexx candidate
To talk one-on-one with one of our team members about how the Regenexx approach may be able to help your orthopedic pain or injury, please complete the form below and we will be in touch with you within the next business day.
References
1, 4. Regenexx Patient Registry – Knee Outcomes. Lower Extremity Functional Scale (LEFS) questionnaire. Accessed on November 02, 2020.
2. Moseley JB, O’Malley K, Petersen NJ, Menke TJ, Brody BA, Kuykendall DH, Hollingsworth JC, Ashton CM, Wray NP. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med. 2002 Jul 11;347(2):81-8. doi: 10.1056/NEJMoa013259. PMID: 12110735. [Google Scholar]
Englund M, Guermazi A, Gale D, Hunter DJ, Aliabadi P, Clancy M, Felson DT. Incidental meniscal findings on knee MRI in middle-aged and elderly persons. N Engl J Med. 2008 Sep 11;359(11):1108-15. doi: 10.1056/NEJMoa0800777. PMID: 18784100. [Google Scholar]
Katz JN, Brophy RH, Chaisson CE, de Chaves L, Cole BJ, Dahm DL, Donnell-Fink LA, Guermazi A, Haas AK, Jones MH, Levy BA, Mandl LA, Martin SD, Marx RG, Miniaci A, Matava MJ, Palmisano J, Reinke EK, Richardson BE, Rome BN, Safran-Norton CE, Skoniecki DJ, Solomon DH, Smith MV, Spindler KP, Stuart MJ, Wright J, Wright RW, Losina E. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N Engl J Med. 2013 May 2;368(18):1675-84. doi: 10.1056/NEJMoa1301408. Epub 2013 Mar 18. Erratum in: N Engl J Med. 2013 Aug 15;369(7):683. PMID: 23506518 [Google Scholar]
Sihvonen R, Englund M, Turkiewicz A, Järvinen TL; Finnish Degenerative Meniscal Lesion Study Group. Mechanical Symptoms and Arthroscopic Partial Meniscectomy in Patients With Degenerative Meniscus Tear: A Secondary Analysis of a Randomized Trial. Ann Intern Med. 2016 Apr 5;164(7):449-55. doi: 10.7326/M15-0899. Epub 2016 Feb 9.PMID: 26856620. [Google Scholar]
van de Graaf VA, Noorduyn JCA, Willigenburg NW, Butter IK, de Gast A, Mol BW, Saris DBF, Twisk JWR, Poolman RW; ESCAPE Research Group. Effect of Early Surgery vs Physical Therapy on Knee Function Among Patients With Nonobstructive Meniscal Tears: The ESCAPE Randomized Clinical Trial. JAMA. 2018 Oct 2;320(13):1328-1337. doi: 10.1001/jama.2018.13308. Erratum in: JAMA. 2018 Dec 4;320(21):2272-2273. Erratum in: JAMA. 2020 Mar 10;323(10):1001. PMID: 30285177. [Google Scholar]
3. Regenexx Patient Registry – Knee Outcomes. Numeric Pain Scale (NPS) questionnaire. Accessed on November 02, 2020.
5. Regenexx Patient Registry – Knee Outcomes. Single Assessment Numeric Evaluation (SANE) questionnaire. Accessed on November 02, 2020.
6. NIH: National Institute of Arthritis and Musculoskeletal and Skin Diseases. Accessed October 5, 2020.
7. Arthritis Foundation. Accessed November 02, 2020.
8. Xia Z, Ma P, Wu N, Su X, Chen J, Jiang C, Liu S, Chen W, Ma B, Yang X, Ma Y, Weng X, Qiu G, Huang S, Wu Z. Altered function in cartilage derived mesenchymal stem cell leads to OA-related cartilage erosion. Am J Transl Res. 2016 Feb 15;8(2):433-46. PMID: 27158337. [Google Scholar]