C1–C2 Screw Fixation: Getting Screwed
These past few years, I have seen an explosion in the number of patients diagnosed with upper cervical instability who are getting C1–C2 screw fixation. This is a surgery that’s a one-way street, like so many, where once you pull the trigger and get the procedure, there’s no going back. Let me explain.
What Is Upper Cervical Instability?
The upper neck is the place where the head meets the spine. The head is held on by tough ligaments, and it’s possible for these ligaments to get injured or become lax due to congenital problems, like Ehler-Danlos syndrome (stretchy ligaments). This can cause excessive motion here known as instability and a myriad of symptoms that include headaches, dizziness, visual problems, rapid heart rate, numbness, and so on.
These patients can be hard to treat. Traditional physical therapy, medications, and pain management injections often don’t help much. Upper cervical chiropractic or specific manual therapy can help many, but for some, the adjustments don’t hold. Other injections, like prolotherapy, PRP, or stem cells, into ligaments (to stabilize the area) can’t reach the deep ligaments. Hence, many patients are left looking at a major surgery.
Upper Cervical Ligaments
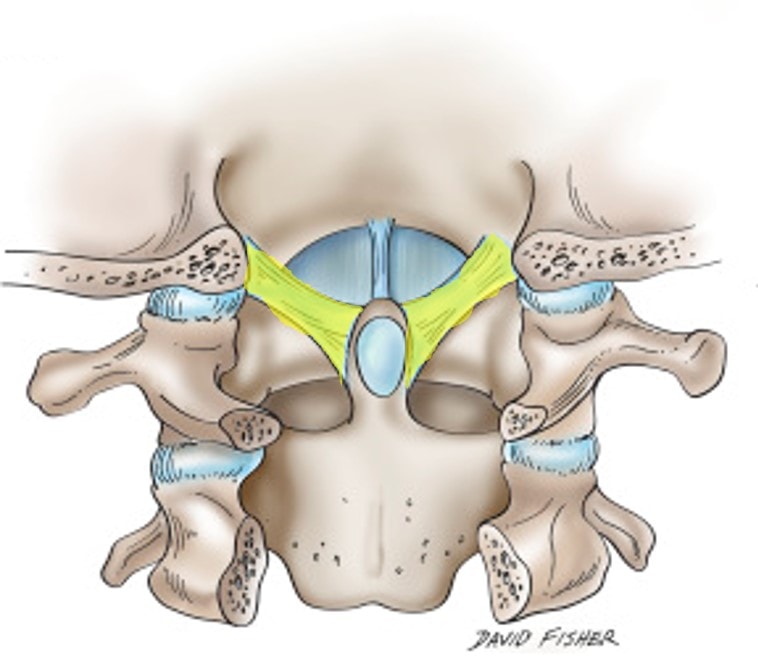
There are lots of upper cervical ligaments that help hold the head on. These include the alar, transverse, and accessory ligaments. The alar ligaments are the ones we’re discussing today. Above, notice (alar ligaments in yellow) that they bind the C2 bone to the skull through the dens (the part of the C2 bone that sticks up). What does this ligament do?

There are neck joints just like you have finger joints. These are held in check from excessive motion by ligaments and the capsules that surround the joints. When the alar ligament becomes loose, this can allow too much motion in the C1–C2 joint as you bend your head to one side or the other. For example, in the image to the left, note that the head and the C1 bone (called the atlas) fall off to the right when the patient bends their head (second diagram). This results in the alignment of the C1 and C2 bones (dashed line), getting messed up.
What Is C1–C2 Screw Fixation?

Yok_onepiece/Shutterstock
One of the major surgeries that can be offered to these patients with loose upper neck ligaments is a craniocervical fusion. This is seen to the left and involves a plate on each side that is screwed into the skull and into the spine. This is a high-risk surgery where the serious complication rate is significant. In addition, the amount of tissue damage that has to be done to accomplish this procedure is extreme. For example, the upper neck muscles are often extensively damaged. To avoid this big cervical surgery, a newer approach is just to place a single screw into the C1–C2 joint. Let’s explore this a bit.
The specific procedure I’m seeing more of is called trans-articular C1–C2 screw fixation.
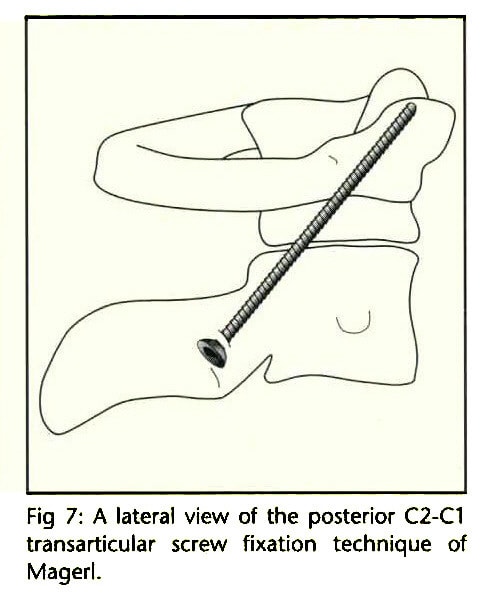
In this procedure, a screw is placed from the back of the neck into the C2 bone, through the C1–C2 joint, and into the C1 bone. The goal is to stabilize the C1 on the C2 bone to take the place of the damaged alar ligaments. The advantage is that this procedure causes less damage to the soft tissues. However, there are also big disadvantages as well. Let’s explore those problems.

First, note that the screw goes through the C1–C2 joint. This is a joint just like the one in your finger, but a bit bigger. It has two bones with cartilage on either end (see diagram above). Hence, when a screw passes through the joint, it creates a hole in both cartilage surfaces (the one on the top and the one on the bottom of the joint).
Getting Screwed: You Can’t Drill a Hole in Cartilage Without Consequences
I’ve spoken to and treated many patients with this type of fusion in place. Why? We offer a novel alar ligament direct technique with bone marrow concentrate (same-day stem cell procedure) with the goal of healing the damaged ligaments to avoid upper neck fusion surgery. What surprises me is that few patients understand the consequences and one-way nature of the surgery. Let me explain.
If you want to create arthritis in a joint in an experimental model, one surefire way to do that is to damage the surface of the cartilage. Hence, drilling a large hole in a joint would be a great way to get there. Hence, this surgery is more likely than not to create arthritis in this joint. That will be less likely to happen as long as the screw stays in place, but if the screw is removed, add in the instability that was there to begin with, and you end up with a joint that quickly becomes arthritic.
The problem? For most patients who have had this surgery, the procedure made them worse once the hardware screws were removed. They don’t seem to understand that the surgeon drilled a large hole in their joint. They also don’t generally understand that removing those screws has consequences.
Is there a way to avoid this surgery? In most patients, the upper neck ligaments can be treated with a precise injection known as the PICL procedure. If this doesn’t work, then you can always get the C1–C2 screw fixation, but unlike the surgery, if it doesn’t work and there are no complications from the injection, there is no problem choosing another path without consequences.
The upshot? Please ask questions about the reversibility of big spine surgery procedures. Many are a one-way street, meaning that once you make the choice to head down a specific pathway, there is no turning back the clock to the way things were before the procedure. That’s the big issue with C1–C2 screw fixation. Once you head down this pathway, there is no heading back.

NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.