The Curious Case of the Typical/Atypical L5-S1 Disc Herniation
In this article:
This week I saw a patient with an L5-S1 disc bulge/herniation who seemed to be a mystery to his physicians but in fact, just had a slightly atypical problem that presented typically. Meaning he seemed to be a mystery in need of a rare diagnosis, but in fact, everything easily lined up if you knew what to look for. Let’s use that story to teach you about the L5-S1 disc.
What Can Happen to the L5-S1 Disc?
Remember that the disc is made up of a thick outer annulus with lots of fibers like the payers of an onion. Also, inside there’s a softer gel that holds onto water (nucleus pulposis).

VectorMine/Shutterstock
So the damage that can happen to an L5-S1 disc all revolve around injuries to the annulus that either allow the nucleus to push out the annular fibers (a disc bulge, protrusion, or prolapse) or squirt out a little (a disc herniation or extrusion) or squirt completely out (disc sequestration).
In the image below, you see a degenerated disc, which is when the annulus gets beat up and the disc lacks the ability to hold onto water and begins to collapse.

Tasty_Cat/Shutterstock
What’s a Subligamentous Disc Herniation?
Running along the backside of the discs is a ligament called the PLL (posterior longitudinal ligament). Think of this as a big piece of duct tape that runs down the back of the spine (in the front of the spinal canal).

Chu KyungMin/Shutterstock
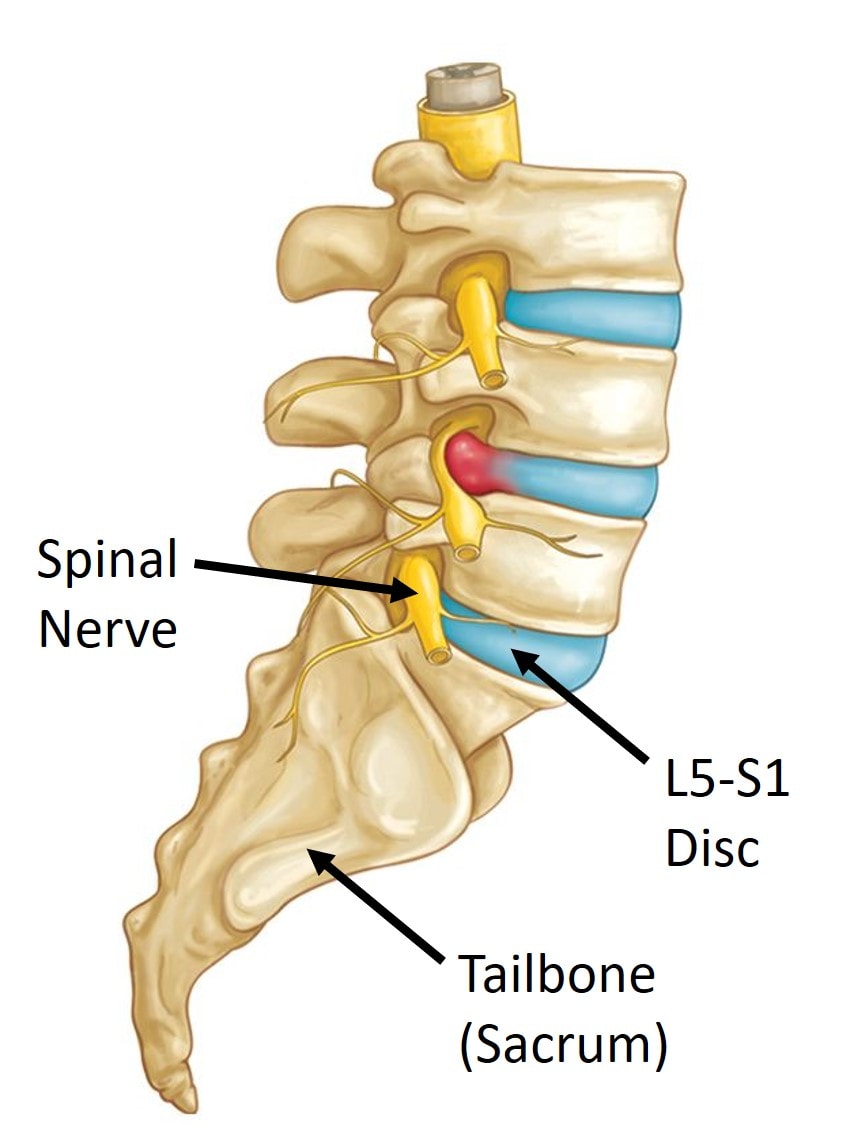
A disc herniation is when the softer gel that lives inside the disc (nucleus pulposis) pushes out through a damaged annulus, the outer covering of the disc. This usually goes to one side or the other of the PLL and comes in contact with the spinal nerves that exit there, which can lead to pain and sciatica.
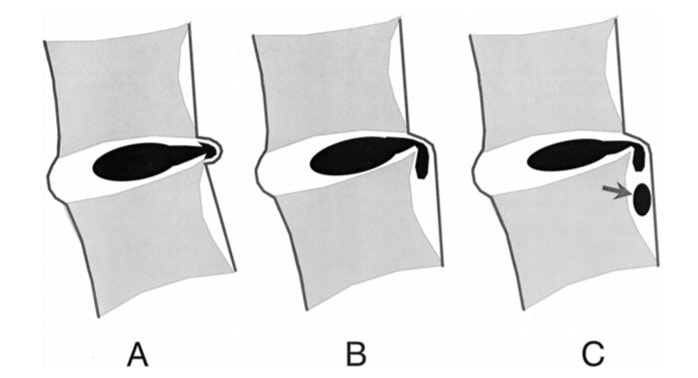
Sometimes the disc herniation happens exactly in the middle of the disc and beneath this ligament (1). When that happens, it’s called a subligamentous disc herniation. In the image below, you can see the different types of central subligamentous disc herniations.
One of the unique things about this type of disc herniation is that often it doesn’t come in contact with the nerves and epidural space. So routine steroid epidurals that should help don’t because the disc is separated from the injected medicine by that PLL.
My patient just graduated from college with an accounting degree, but last year, he began to notice back pain with numbness and tingling at the bottom of his foot. He eventually had an MRI that showed the same type of subligamentous disc herniation that I describe above. He quickly had an epidural by out-of-state physicians and they seemed puzzled that he didn’t respond. So let’s dig into why the epidural didn’t work for him.
What Is an Epidural?
Epidural steroid injections have become a mainstay of treatment for herniated discs and back pain caused by the L5-S1 disc (2). This is where the doctor takes a needle and guides it using real-time x-ray guidance into the area between the disc and the spinal nerve. He or she then injects radiographic contrast to ensure that the medication will go into the epidural space. Then a high-dose steroid medication and anesthetic is injected.
The good news is that since this is a potent anti-inflammatory medication, sciatica and back pain usually quickly diminish. However, there are downsides to this treatment approach that have caused us to use a different approach, which I’ll discuss below. However, for this patient, he didn’t get the typical result. Why?
Remember when I said his disc was under that PLL ligament? Since his disc material didn’t communicate with the epidural space, the medication injected into that space couldn’t act on that spot. Hence, he got minimal relief from his back pain. Regrettably, his local doctors didn’t recognize this which caused them to do more injections that weren’t needed.
What Are the Symptoms of an L5-S1 Disc Bulge or Herniation?
Sir William Osler, one of the fathers of modern medicine once said that if you listen to the patient long enough they’ll tell you the diagnosis. What he meant is that we doctors like to talk over our patients thinking we know it all, but if we just did more listening than talking, our patients would make our job easy. That was exactly this situation as this kid told me he had an L5-S1 disc problem, but his other doctors back in Nebraska weren’t listening.
After he didn’t respond to the epidural, his doctors began to get all sorts of other tests and began injecting more things including his SI joint and low back discs (discogram). However, here’s what he told me were his symptoms which are all related to his L5-S1 disc problem:
- Numbness in the leg that went to the bottom of the foot. This is the S1 nerve which would be expected to be irritated by a central L5-S1 disc herniation. Numbness can also go to the big toe had his disc been out more to one side, which would be the L5 spinal nerve.
- Pain/tightness in the hamstrings, side of the leg, and calf. These are all muscles or areas connected to muscles (like the iliotibial band or ITB) that connect back up to the S1 nerve.
- When I pushed on his vertebrae on an exam, the only one that causes pain is L5-S1.
So he’s telling me that this L5-S1 disc herniation is causing his problem.
What Happens When an Epidural Doesn’t Work?
As I said above, his doctors were thrown for a loop when he didn’t respond to the epidural (which he shouldn’t have responded to because of the location of his L5-S1 disc herniation), but they were positively apoplectic when he started to get new pain going up to his ribs. Yet this was to be expected had they understood simple low back pain biomechanics. Let me explain.
When you have an L5-S1 disc bulge or herniation, that irritates the local L5 or S1 spinal nerves. Some parts of these nerves go down the leg causing sciatica. However, other parts head back toward the spine and tell the local multifidus muscles what to do. These muscles are deep spinal stabilizers that are critical for keeping the spine bones aligned while you move. Long-term nerve irritation of those spinal nerves cause atrophy and shrinkage of the low back multifidus muscles (3). What happens next is predictable.
Once those multifidus muscles shrink and the L5 vertebra begins getting sloppy uncontrolled movement, the body kicks in the big low back muscles to try and tighten everything down. The goal is to provide rigidity to the whole system which stops some of the sloppy motion ta L5. Patients often feel this as a back spasm. However, these big muscles aren’t designed to stay tight for very long, so eventually, they get tired and their tendons get beat up causing a new problem called tendinopathy.
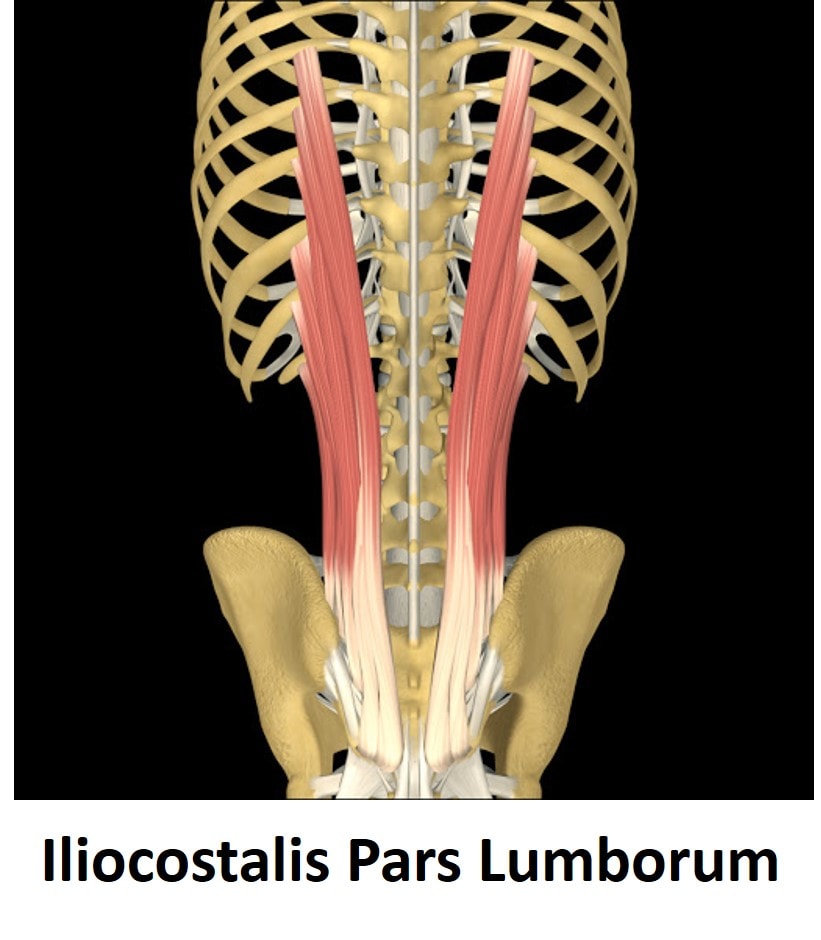
Which big spine muscle was causing his problem? It’s called the iliocostalis pars lumborum as shown below. It goes from the pelvis to the back of the ribs. This is why he felt new pain developing from his back to the back part of his ribs. This was to be expected due to the multifidus atrophy that was clearly seen on his MRI, but not read out by the reading radiologist. This is why his doctors ordered a completely unnecessary thoracic MRI.
How Do You Treat an L5-S1 Disc Herniation?
This patient drove from Nebraska to our Colorado HQ to get answers that his local doctors didn’t have. What can we do differently?
First, we no longer use high-dose steroids for epidurals. Instead, we use the patient’s growth factors isolated from their blood platelets or what’s called platelet lysate (4). Why do we inject that epidural rather than high-dose steroids? The steroids damage local tissue, while platelet growth factors can help to repair tissue and they can also manage inflammation for longer. See my video below:
Next, if that doesn’t work, then we will inject high-dose PRP (plasma rich platelets) into his disc, as that will access the damaged area that doesn’t communicate with his epidural space. While his prior doctors did a test like that called a discogram, they failed to inject anything that could help repair the disc. To see what that procedure looks like, see my video below:
Finally, his multifidus is also atrophied, so we’ll inject that using ultrasound guidance with PPP (Platelet Poor Plasma) as that’s been shown in studies to be better at muscle repair. We’ll also use ultrasound guidance to inject the damaged tendons of his iliocostalis muscle.
The upshot? At the end of the day, this patient has a typical L5-S1 disc problem that presented the normal way, but because it’s in a little atypical position, under the PLL ligament, he didn’t respond to epidural injections. That led his physicians on a wild goose chase because they never listened to him long enough for him to tell them what was wrong. They also lacked the experience to see how his problem was developing and how to treat it with regenerative medicine techniques.
_______________________________
References
(1) Appel B. Nomenclature and classification of lumbar disc pathology. Neuroradiology. 2001 Dec;43(12):1124-5. doi:10.1097/00007632-200103010-00006
(2) Pena E, Moroz L, Singh D. Lumbar Epidural Steroid Injections. JBJS Essent Surg Tech. 2016;6(3):e25. doi:10.2106/JBJS.ST.O.00058
(3) Freeman MD, Woodham MA, Woodham AW. The role of the lumbar multifidus in chronic low back pain: a review. PM R. 2010 Feb;2(2):142-6. doi:10.1016/j.pmrj.2009.11.006
(4) Centeno C, Markle J, Dodson E, et al. The use of lumbar epidural injection of platelet lysate for treatment of radicular pain. J Exp Orthop. 2017;4(1):38. doi:10.1186/s40634-017-0113-5

NOTE: This blog post provides general information to help the reader better understand regenerative medicine, musculoskeletal health, and related subjects. All content provided in this blog, website, or any linked materials, including text, graphics, images, patient profiles, outcomes, and information, are not intended and should not be considered or used as a substitute for medical advice, diagnosis, or treatment. Please always consult with a professional and certified healthcare provider to discuss if a treatment is right for you.